
The IOM has issued it's report on diagnostic errors which I believe highlights highlights major issues in the diagnostic realm. I have not had a chance to review it completely but I have been involved with the Society for Improved Diagnosis in Medicine (SIDM). I have heard much of discussions leading up to the report and have devoted much thought to problems in diagnosis.
One colleague in Pathology whose thinking and writings have influenced me greatly in this realm is Dr. Elliott Foucar who for more than 20 years highlighted the limitations of anatomic pathology is the diagnostic sphere. One key concept that he highlighted is that pathology made a transition in the 20th century from being a taxonomic activity to being engaged in the assessment of risk. I now have come to realize that the remainder of medicine has followed in the transition without having grasped that the transition has occurred. The SIDM and the IOM have delved into this world without explicitly recognizing the relevance of this concept to the act of making a diagnosis.
What Dr. Foucar has written about is how anatomic pathology at it origins focused on the autopsy with the sole purpose of identifying characteristics of disease which caused someone's death. An autopsy of a woman with a breast mass might identify a tumor with a specific histology and evidence of tumors elsewhere. This information was subsequently used to make predictions about live individuals who shared certain characteristics with someone already dead. For example, a live woman might present with a ulcerated 5 cm breast mass which when samples demonstrated a tumor with great similarity to what had already been observed in patients on the autopsy table. In contrast, another live woman might present with a similar mass which was showed a cyst and inflammatory cells. Histology was an amazingly powerful tool which allowed for clear separation of these distinct entities. What anatomic histology functioned as here is as a taxonomic tool, separating a being inflammatory process from a clearly malignant one. Diagnosing a ulcerated breast cancer as an infected cyst would be a clear diagnostic error, misidentifying one entity with a almost certain malignant course as a distinct entity with a benign clinical course.
Fast forward to the 21st century. Now instead of attempting to distinguish distinct clinical entities with distinct pathologies, anatomic pathology tries to separate infinite grades of dysplasias from forms of actual cancer. There is no clear line which can separate low grade dysplasias from high grade dysplasias; scoring systems are riddled with subjectivity and inconsistencies, whether the tissues are breasts, prostates, or pigmented lesions of skin, The life expectancy of those diagnosed with dysplastic lesions tend to be identical to those diagnosed with malignancies.
The transition which has occurred is one where the pathologist has moved from being a taxonomist to being an actuary. Actuaries use information to identify people or groups who are at risk for certain outcomes. Their functions are essential for certain financial entities such as insurance companies which need to put money aside to cover costs which might occur when particular events occur such as floods, fire, or illness. They assign specific odds for such events in particular populations.
In many respects, diagnoses are always actuarial statements. Someone who presents with chest pain, shortness of breath, an abnormal EKG, and positive cardiac muscle enzymes almost certainly is having an acute myocardial infarction. This carries with it the immediate morbidity but the diagnosis has a prediction about the future built into it as well. Those affected are at near immediate risk for death. This is a prediction one does not need to wait around for months or years to assess. The acute MI diagnosis is an actuarial statement of short term outcomes.
A host of tools within the cardiovascular realm have purported to extend the ability to predict future outcomes much further into the future. We can image the coronary circulation using a variety of tools. However, moving the time frame for the predictions creates all sorts of problems, both practical and conceptually. For a patient who has clear cardiac symptoms and functional impairment short of what qualifies as an acute MI, imaging tools may allow for predictions in the non-acute time frame. However, there are efforts to push out the time windows for predictions out into years or even decades into the future. Conceptually, do "abnormal" findings observed from studies of asymptomatic individuals represent distinct diseases or diagnoses or do they represent risk factors? What represents an abnormality if the finding is common within the population studied?
Our ability to peer inside of people now is unprecedented. Whether we peer using ultrasound, x-rays, CAT scans, MRI scans, or PET scans, we can literally visualize and see what could not previously be seen unless someone was cut open on the operating table. A recent story published in the New York Times discussed new observations regarding the use of scans looking for calcification of coronary arteries. The absence of calcium seem to predictive of much lower risk of cardiac events in a 10 year time line than what conventional risk calculators might suggest. However, questions were raised because of the nearly 5% incidental findings on scan. The reality is we don't know what the range of normal findings might look like. Similarly, the ability to do ultrasound on thyroids has led to an epidemic of thyroid biopsies. We are about to embark on widespread CAT scans to detect lung cancers, most of which are likely to be indolent.
As we peer at and into into people with tools of increasing resolution and sensitivity, we will see things. Whether the things we observe will represent variations with little or not relevance to future outcomes, or whether they will represent abnormalities which place a given patient at risk for a bad outcomes will be asked. The temptation will always be there to view anything out of the ordinary as a reason to act. As the tools get more sensitive, the opportunities to observe variations will become overwhelming. When will we recommend acting and when will we write variations off as simply variations? Like screenings at the airport and those working at homeland security, we will have to deal with rare signals within a sea of noise. Ideally, we can become like actuaries, if we can accumulate enough solid data to allow us to make data driven decisions. Until then, we will make our decisions driven by fear and complacency.
Sunday, December 13, 2015
What the electronic medical record has revealed about health care delivery
I have and am living through the deployment of the electronic medical record (EHR) within the health systems I am employed by. It is something that will continue to evolve for the remainder of my practice lifetime and beyond. Stories regarding EHR deployment have tended to focus either on the pain involving end users or the promise of implementation. There is no question whatsoever that EHR deployment has been disruptive and has had unintended consequences on the delivery of health care services. I would also suggest that it has been revealing of aspects and elements of health care delivery of which we had very limited awareness.
That the movement of operations from paper based to electronic information systems ends up revealing novel aspects of the business of health care should not come as a surprise. Virtually all industries which have made this transition have undergone similar realizations. Archaic legacy processes which were hidden and not measurable become revealed and quantified. Value added activities become separable from non-value added actions. Management, which was previously driven by intuitive decision making can move toward data driven decisions.
Medicine is not one industry and the habit we have to lump all health care activities into one bucket has really obscured the nature of the challenges we face, especially relating to the movement to digital information systems. My perspective is by its very nature narrow, colored by the fact that I am physician and a sub specialty doctor to boot. However, even within the narrow universe of physician perspectives, the differences within even this narrow scope dwarf the similarities. Some physicians are primarily technicians who view their jobs are doing very narrowly defined tasks. These might include replacement of a joint, removal of a specific tumor, insertion of a stent, or repair of a hernia in a given person at a given time. For a physician who performs this type of service, the information which comes out of the EHR or for them to enter into the EHR is very focused on their specific value added service.
In contrast, other physicians manage chronic conditions over extended periods of time. Some of these doctors (or APPs) may be generalists while some may be specialists. The role of the EHR under these circumstances is completely different from the role it plays for the technician providers, both from the perspective of what any given physician needs to extract to make effective decisions and from the perspective of what needs to be entered into EHRs at any given moment of time. If a patient has multiple chronic medical problems which all need to be simultaneously managed, the quality of the inputs and the ability to digest information over time ultimately determines the quality of the care delivered and the outcomes achieved.
If one asks practitioners who primary focus is acute interventions what value is added by the EHR and how this can be improved, you will get very different answers than if you ask physicians whose primary focus is long term care, including disease prevention and chronic disease management. The answers will be so different that you can't help but conclude that these groups are engaged if distinctly different industries. That is my point. We are not deploying the EHR in one industry, but in reality multiple different industries lumped inappropriately under one roof. To believe the EHR needs of an orthopedic surgeon who primarily replaces knees will overlap significantly with an allergist who primarily manages chronic asthma, or a primary care physician who manages many problems over time is delusional. The EHR is ideally an information management tool and both the types and perhaps more importantly the flows of information required by different practitioners is completely different. Both airline pilots and diesel mechanics are involved in the transportation industry but they require very different information sets to do their jobs. Similarly, whether one is dealing with an acute with an acute issue or a chronic issue in health care delivery will mean that what information one needs to address a particular problem or problems will be very different.
Obscuring this reality has been the dramatic change in medicine which has occurred in the past 50-75 years. When my parents were growing up, for most people one went to a physician when one was very sick and the the measure of success was whether you were dead within days to at most weeks. Information systems were not essential. There were not many drugs that patients took chronically and the outcome measurement was relatively simple; your were either dead or not dead. Decisions regarding optimal management were primarily intuitive and not dependent upon sophisticated information systems.
Fast forward to the year 2015 and much had changed. While the healthcare delivery system still deals with acute and life threatening issues, many if not most encounters with health systems and providers deal with chronic issues managed over long term time lines of years to decades. However, we are still locked into a very similar delivery model as was used 75 years ago. Furthermore, while we pay lip service to evidence based medicine, we still operate primarily on an intuitive level. We have no choice since within the outpatient delivery realm, our information systems are so dismal that we are left with few other options. We measure money in and out and don't do this so well.
The culture where we value intuitive master clinicians creates another challenge in that when software engineers were developing the current first generation EHR tools. There were few clinicians who actually had substantial understanding of what information they needed to make decisions. Little effort was made to engage front line clinicians in the design of EHRs but when it was made, few front line personnel had any idea of what to tell EHR developers. In the absence of a significant cadre of clinicians who practiced in an information driven manner, there was no one to effectively guide the EHR development process away from where it went. We created billing justification tools because that is where we could define where information made a difference.
For the most part, measurements of things which reflect activities that might add value to patient's lives were few and far between. Efforts are being made to figure out how to measure what is important and measure whether resources invested to deliver specific services are worth the cost. However, the going is slow. Standardization and measurement is hard work and meets resistance for a host of reasons. One particular problem is that activities which are the financial foundations of practice may in fact generate very limited value to patients. What we as physicians may view as valuable may not be viewed so positively by the recipients of our care. We are very likely to experience surprises as physician centric universe moves more and more toward a patient centric one.
That the movement of operations from paper based to electronic information systems ends up revealing novel aspects of the business of health care should not come as a surprise. Virtually all industries which have made this transition have undergone similar realizations. Archaic legacy processes which were hidden and not measurable become revealed and quantified. Value added activities become separable from non-value added actions. Management, which was previously driven by intuitive decision making can move toward data driven decisions.
Medicine is not one industry and the habit we have to lump all health care activities into one bucket has really obscured the nature of the challenges we face, especially relating to the movement to digital information systems. My perspective is by its very nature narrow, colored by the fact that I am physician and a sub specialty doctor to boot. However, even within the narrow universe of physician perspectives, the differences within even this narrow scope dwarf the similarities. Some physicians are primarily technicians who view their jobs are doing very narrowly defined tasks. These might include replacement of a joint, removal of a specific tumor, insertion of a stent, or repair of a hernia in a given person at a given time. For a physician who performs this type of service, the information which comes out of the EHR or for them to enter into the EHR is very focused on their specific value added service.
In contrast, other physicians manage chronic conditions over extended periods of time. Some of these doctors (or APPs) may be generalists while some may be specialists. The role of the EHR under these circumstances is completely different from the role it plays for the technician providers, both from the perspective of what any given physician needs to extract to make effective decisions and from the perspective of what needs to be entered into EHRs at any given moment of time. If a patient has multiple chronic medical problems which all need to be simultaneously managed, the quality of the inputs and the ability to digest information over time ultimately determines the quality of the care delivered and the outcomes achieved.
If one asks practitioners who primary focus is acute interventions what value is added by the EHR and how this can be improved, you will get very different answers than if you ask physicians whose primary focus is long term care, including disease prevention and chronic disease management. The answers will be so different that you can't help but conclude that these groups are engaged if distinctly different industries. That is my point. We are not deploying the EHR in one industry, but in reality multiple different industries lumped inappropriately under one roof. To believe the EHR needs of an orthopedic surgeon who primarily replaces knees will overlap significantly with an allergist who primarily manages chronic asthma, or a primary care physician who manages many problems over time is delusional. The EHR is ideally an information management tool and both the types and perhaps more importantly the flows of information required by different practitioners is completely different. Both airline pilots and diesel mechanics are involved in the transportation industry but they require very different information sets to do their jobs. Similarly, whether one is dealing with an acute with an acute issue or a chronic issue in health care delivery will mean that what information one needs to address a particular problem or problems will be very different.
Obscuring this reality has been the dramatic change in medicine which has occurred in the past 50-75 years. When my parents were growing up, for most people one went to a physician when one was very sick and the the measure of success was whether you were dead within days to at most weeks. Information systems were not essential. There were not many drugs that patients took chronically and the outcome measurement was relatively simple; your were either dead or not dead. Decisions regarding optimal management were primarily intuitive and not dependent upon sophisticated information systems.
Fast forward to the year 2015 and much had changed. While the healthcare delivery system still deals with acute and life threatening issues, many if not most encounters with health systems and providers deal with chronic issues managed over long term time lines of years to decades. However, we are still locked into a very similar delivery model as was used 75 years ago. Furthermore, while we pay lip service to evidence based medicine, we still operate primarily on an intuitive level. We have no choice since within the outpatient delivery realm, our information systems are so dismal that we are left with few other options. We measure money in and out and don't do this so well.
The culture where we value intuitive master clinicians creates another challenge in that when software engineers were developing the current first generation EHR tools. There were few clinicians who actually had substantial understanding of what information they needed to make decisions. Little effort was made to engage front line clinicians in the design of EHRs but when it was made, few front line personnel had any idea of what to tell EHR developers. In the absence of a significant cadre of clinicians who practiced in an information driven manner, there was no one to effectively guide the EHR development process away from where it went. We created billing justification tools because that is where we could define where information made a difference.
For the most part, measurements of things which reflect activities that might add value to patient's lives were few and far between. Efforts are being made to figure out how to measure what is important and measure whether resources invested to deliver specific services are worth the cost. However, the going is slow. Standardization and measurement is hard work and meets resistance for a host of reasons. One particular problem is that activities which are the financial foundations of practice may in fact generate very limited value to patients. What we as physicians may view as valuable may not be viewed so positively by the recipients of our care. We are very likely to experience surprises as physician centric universe moves more and more toward a patient centric one.
Saturday, October 10, 2015
It's the payment system, stupid
It have taken a long hiatus from writing. I am not sure why. Part of the reason may be I have been so busy with work. Part of the reason has also been the world is so confusing that I did not believe I could say anything useful or coherent. Finally, writing required that I sit in front of a computer for even more time. My Fitbit has prompted me to get up and move. When I move, I don't write. Perhaps I need to buy a walking computer desk. Sounds dangerous...
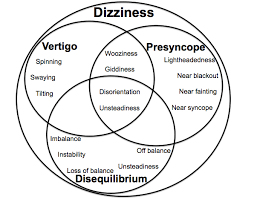 I had a conversation with one of my colleagues at work this week which got me to thinking. He was a former ENT physicians who rose to leadership positions. He remarked that when he ran his department, there were always patients with particular diseases whom no one wanted to care for. For ENT these were the dizzy patients. No one wanted to see the dizzy patients. There was no shortage of calls for help. There are lots of dizzy people who are simply miserable with their disorder (the 12 month prevalence may be as high as 5%), but a limited to non-existent workforce who want to treat these afflicted individuals.
I had a conversation with one of my colleagues at work this week which got me to thinking. He was a former ENT physicians who rose to leadership positions. He remarked that when he ran his department, there were always patients with particular diseases whom no one wanted to care for. For ENT these were the dizzy patients. No one wanted to see the dizzy patients. There was no shortage of calls for help. There are lots of dizzy people who are simply miserable with their disorder (the 12 month prevalence may be as high as 5%), but a limited to non-existent workforce who want to treat these afflicted individuals.
 This is not specific to ENT and dizzy patients. For dermatologists, there are the itchy patients; for the rheumatologists the fibromylagia patients; for the gastroenterologists it is the irritable bowel syndrome patients; for the neurologists it is patients with headaches; for the hemologists/oncologists it is anyone who does not have cancer; for the orthopedists it is patients who have back pain who are not operative candidates. There are common and awful conditions which may be terribly debilitating. Yet it is common knowledge that the care community view these entities as one might view the old maid card in the card game. One is best served by passing this off to someone else.
This is not specific to ENT and dizzy patients. For dermatologists, there are the itchy patients; for the rheumatologists the fibromylagia patients; for the gastroenterologists it is the irritable bowel syndrome patients; for the neurologists it is patients with headaches; for the hemologists/oncologists it is anyone who does not have cancer; for the orthopedists it is patients who have back pain who are not operative candidates. There are common and awful conditions which may be terribly debilitating. Yet it is common knowledge that the care community view these entities as one might view the old maid card in the card game. One is best served by passing this off to someone else.
 What all of these things have in common is that they are common entities, rarely life threatening, may be difficult to treat, and most importantly, their value in the medical payment lottery has been arbitrarily set below where it provides incentives for health care professionals offer care to patient afflicted. The payment system has created huge disincentives for physicians and health systems to offer services to patients with these common and debilitating (but non-lethal) conditions.
What all of these things have in common is that they are common entities, rarely life threatening, may be difficult to treat, and most importantly, their value in the medical payment lottery has been arbitrarily set below where it provides incentives for health care professionals offer care to patient afflicted. The payment system has created huge disincentives for physicians and health systems to offer services to patients with these common and debilitating (but non-lethal) conditions.
In virtually all other sphere of human endeavors, unmet human needs and wants create opportunities for people and businesses to grow wealthy by stepping to meet human needs. This is not so much true within health care. The convergence of top down administrative pricing schemes and restrictive and punitive participation rules has created a sorry state which has basically orphaned huge segments of care needs. Let's say I am a neurologist who might have an interest in the care of patients with chronic headaches. The estimates are that this symptom affects about 50% of the population in any given year and 3% have chronic disease (meaning > 15 days per month - about 10 million people!). If I follow evidence based guidelines, I will find managing these patients a financially losing proposition because the payment system (E&M codes primarily) arbitrarily assigns payments below the level of cost of delivery of service. As a rational person, I leave this business.
In other businesses, the shortage of supply allows remaining players to adjust the price of service to the point where continued delivery of services can be maintained or grown to meet needed demand. In health care, prices are fixed and almost impossible to respond to unmet demand. Yes, one could consider pulling out from Medicare or private contracts but it is much lower risk to simply offer other services which pay much better.

For the patients who have headaches, non-specific GI discomfort, itching, dizziness, fibromylagia, or similar states who get through the filters into your office, they will not likely come back if the level of service is sufficiently dismal. Whether intentional of not, there are benefits from the deployment of strategic clinical incompetence. Thus, there has been a wholesale exodus from providing care to patients with a host of very troubling, uncomfortable, debilitating and remarkably common conditions. No wonder the alternative medicine industry has moved in to fill this void.
 Leadership within the conventional health care ranks are blind to much of this. To keep your health care delivery teams happy and financially healthy, it is essential to keep these patients out of your system as much as possible. One is best served not to give much thought to the origins of this issue.
Leadership within the conventional health care ranks are blind to much of this. To keep your health care delivery teams happy and financially healthy, it is essential to keep these patients out of your system as much as possible. One is best served not to give much thought to the origins of this issue.
Look at virtually any medical office or system's website and you will see various offerings of what that group is marketing to the public. I reviewed the Mayo clinic site and typed in a series of symptoms or conditions. When I typed in chest pain, joint replacement, or cancer, I got an informational site which had a "request appointment" button. When I typed in headache, itching, or dizziness, I got information but no opportunity to request an appointment. How interesting....
However, the movement toward consumer driven care may unmask this problem. I think it is only a matter of time before the public becomes aware of the disconnect between what we are incentivized to do and want to do currently and what unmet needs exist. My concern is that the response will be heavy handed, top down, and will double down on the current dysfunctional payment system. It will create just a new set of winners and losers based upon political games.
In virtually all other sphere of human endeavors, unmet human needs and wants create opportunities for people and businesses to grow wealthy by stepping to meet human needs. This is not so much true within health care. The convergence of top down administrative pricing schemes and restrictive and punitive participation rules has created a sorry state which has basically orphaned huge segments of care needs. Let's say I am a neurologist who might have an interest in the care of patients with chronic headaches. The estimates are that this symptom affects about 50% of the population in any given year and 3% have chronic disease (meaning > 15 days per month - about 10 million people!). If I follow evidence based guidelines, I will find managing these patients a financially losing proposition because the payment system (E&M codes primarily) arbitrarily assigns payments below the level of cost of delivery of service. As a rational person, I leave this business.
In other businesses, the shortage of supply allows remaining players to adjust the price of service to the point where continued delivery of services can be maintained or grown to meet needed demand. In health care, prices are fixed and almost impossible to respond to unmet demand. Yes, one could consider pulling out from Medicare or private contracts but it is much lower risk to simply offer other services which pay much better.
For the patients who have headaches, non-specific GI discomfort, itching, dizziness, fibromylagia, or similar states who get through the filters into your office, they will not likely come back if the level of service is sufficiently dismal. Whether intentional of not, there are benefits from the deployment of strategic clinical incompetence. Thus, there has been a wholesale exodus from providing care to patients with a host of very troubling, uncomfortable, debilitating and remarkably common conditions. No wonder the alternative medicine industry has moved in to fill this void.
Look at virtually any medical office or system's website and you will see various offerings of what that group is marketing to the public. I reviewed the Mayo clinic site and typed in a series of symptoms or conditions. When I typed in chest pain, joint replacement, or cancer, I got an informational site which had a "request appointment" button. When I typed in headache, itching, or dizziness, I got information but no opportunity to request an appointment. How interesting....
However, the movement toward consumer driven care may unmask this problem. I think it is only a matter of time before the public becomes aware of the disconnect between what we are incentivized to do and want to do currently and what unmet needs exist. My concern is that the response will be heavy handed, top down, and will double down on the current dysfunctional payment system. It will create just a new set of winners and losers based upon political games.
Sunday, May 10, 2015
Proliferating Rules and Diminishing Returns
 A good friend of mine forwarded a link to Charles Murray's piece in the WSJ yesterday titled "Regulation Run Amok- And How to Fight Back" (Rules Run Amok). He knew that the article would pique my interest and he was right. It is a preview of part of a larger work which is to be published shortly, a book called "By the People: Rebuilding Liberty Without Permission". I will need to read this. However, I suspect I may have some basic disagreements with the author.
A good friend of mine forwarded a link to Charles Murray's piece in the WSJ yesterday titled "Regulation Run Amok- And How to Fight Back" (Rules Run Amok). He knew that the article would pique my interest and he was right. It is a preview of part of a larger work which is to be published shortly, a book called "By the People: Rebuilding Liberty Without Permission". I will need to read this. However, I suspect I may have some basic disagreements with the author.The premise of the article is that the regulatory state is out of control, a contention that I wholeheartedly agree with. However, he goes on to suggest that the regulated have an inherent advantage over the regulators, given sheer numbers. He contends that the regulatory state is analogous to a regulatory Wizard of Oz, appearing all powerful but in reality being relatively weak, like the old man behind the curtain. I think he has got this all wrong.
The proliferation of rules backed up by the regulatory power of the state is a set up for use of arbitrary power, which can and will be wielded by the worst of humanity. This sort of environment will and does serve as a magnet for those with the worst of intentions, who see the potential for power and control. Yes,, there might not be sufficient resources to enforce rules effectively and consistently. However, that will not longer be the purpose of any of this. Rules will be enforced to yield the maximum of power to a different end; personal gain for those who have placed themselves in strategic positions to benefit from selective application of rules. This is a story as old as mankind.
In my opinion, the regulatory state run amok has its origins in acceptance of a set of assumptions which now goes increasingly unchallenged. We see challenges in how people fare in our world and we look for solutions. People are poor. People get sick. People treat other people poorly. People foul their environments. We have a host of tools to address these situations, either as individuals or as groups. We can use persuasion or we can use coercion to nudge or shove other people or groups to behave in such a way to improve their own lots or the lots of others.

Our current situation has grown out of the mistaken belief that when a problem arises, the best and increasingly only way to address any and all problems is via state politics. See a problem and pass a law. However, not all problems are amenable to legal redress. The law is a blunt instrument based upon the assumption that the best way to get people to do something is to hold a gun to their heads, using the coercive power of the state to force them to behave in particular ways.
Almost 20 years ago, Richard Epstein wrote an incredibly insightful book "Simple Rules for a Complex World". I have cited this book many times in this blog. It was perhaps the book which has influenced my thinking more than any other book I have ever read. What he presents in this book are a compelling set of arguments for why we should not default to increasingly complex rules, especially legal rules, to optimize a world dependent upon humans working together. The concepts are actually relatively simple. Not all problems require action, particularly legal action. Isolated bad outcomes are compatible with good systems. Not all additional legal interventions result in better outcomes.
Once one starts down the road where every single undesirable outcome serves as the basis of some additional intervention in the form of increasingly complex rules, it leads to a cascade of creation of new rules which create worse outcomes which then serves as the basis of even more rules. While ignoring the rules may seem like a workable solution, I am VERY skeptical that this will yield anything more than individual short term gains at the cost of the creation of contempt for all rules, both functional and non-functional. That sounds like a strategy to optimize one's circumstances immediately before the onset of chaos.
Sunday, April 19, 2015
Who coordinates the coordinators?
This is the first line of an article written by Paula Span and published this week in the New York Times (the-tangle-of-coordinated-health-care). It is good news that there is a recognition that coordination of care is an important and up to now under recognized element(s) of the delivery of care. However, it should come as no surprise that the simple recognition and allocation of modest sums of funds should not solve the coordination problem.
Second to and perhaps equal to the development of technology, the ability of humans to work together to address problems and delivery of human wants and needs is one of the greatest achievement of humankind. I am reminded of the first chapter of the book, Microeconomics by Samuel Bowles where he describes traveling into a rural area of southern India to the village of Palanpur. He wrote:
The time, money and effort allocated to health care delivery has basically exploded within our economy over the past 70 years. The amount of money which has been invested in systems to coordinate care has been vastly outstripped by the investment to simply do more things, whether that be delivery of drugs, surgery, or other discrete interventions. The primary purpose of the payment mechanisms deployed to deliver these services has been to insulate the consumers from the cost of those services, not to assure that interventions are effective or wise.
Furthermore, this system underwent extraordinary expansion at the very time where a concurrent expansion in wealth and productivity was also experienced. Thus, this allocation and investment in health care services was not held to the same standards used to assess the wisdom of investment. By insulating the public of the cost, at least in the short term, they were not sensitive to whether this investment was a good investment in their needs and wants. They received a product(s) which appeared to be worth their investment, the size and scope of which they were blissfully unaware.
The lack of investment in coordination of services virtually guarantees that there are huge elements of waste. Because we experienced such dramatic economic growth, the magnitude of that waste could be masked, at least for a while. We are now reaching the point to where that waste cannot be hidden and business as usual cannot go on. However, how does one create effective coordination within a business which has undergone extraordinary growth in both size and scope when so little investment was made in coordination infrastructure?
The issue is not so unique, as noted by Dr. Bowles above. It is foundational to the effective development of any system which delivers basically any product or service to large numbers of people and is integral to any system with depends upon the specialization of labor. This is not a problem, the details of which will yield to proscriptive human efforts and planning, working off some master human plan. The track record of this approach has a perfect batting average, that being perfectly awful and uniform failure.
The title of the subheading immediately prior to the paragraph above in Dr. Bowles book is labeled simply "Getting the rules right". What are those rules which create the correct incentives which allow for complex systems which effectively coordinate human activities? Note that the rules to achieve this are not likely unique to health care environments and we just as likely to gain insights from circumstances divorced from health care delivery than from within.
Given this historical context, the thought that Medicare or some other insurer could fix this problem by creation of a handful of billing codes to pay for "care coordination" is essentially laughable. The fact that a host of disconnected delivery entities has created new coordination issues in their attempts to fix care coordination problems should come not as a surprise.
Second to and perhaps equal to the development of technology, the ability of humans to work together to address problems and delivery of human wants and needs is one of the greatest achievement of humankind. I am reminded of the first chapter of the book, Microeconomics by Samuel Bowles where he describes traveling into a rural area of southern India to the village of Palanpur. He wrote:
Like the overnight train that left me in an empty field some distance from the settlement, the process of economic development has for the most part bypassed the two hundred or so families that make up the village of Palanpur. They have remained poor, even by Indian standards: less than a third of the adults are literate, and most have endured the loss of a child to malnutrition or to illnesses that are long forgotten in other parts of the world. But for the occasional wristwatch, bicycle, or irrigation pump, Palanpur appears to be a timeless backwater, untouched by India’s cutting edge software industry and booming agricultural regions. Seeking to understand why, I approached a sharecropper and his three daughters weeding a small plot. The conversation eventually turned to the fact that Palanpur farmers sow their winter crops several weeks after the date at which yields would be maximized. The farmers do not doubt that earlier planting would give them larger harvests, but no one the farmer explained, is willing to be the first to plant, as the seeds on any lone plot would be quickly eaten by birds. I asked if a large group of farmers, perhaps relatives, had ever agreed to sow earlier, all planting on the same day to minimize losses. “If we knew how to do that,” he said, looking up from his hoe at me, “we would not be poor.”--Samuel Bowles, Microeconomics: Behavior, Institutions, and Evolution, pp. 24-25
The time, money and effort allocated to health care delivery has basically exploded within our economy over the past 70 years. The amount of money which has been invested in systems to coordinate care has been vastly outstripped by the investment to simply do more things, whether that be delivery of drugs, surgery, or other discrete interventions. The primary purpose of the payment mechanisms deployed to deliver these services has been to insulate the consumers from the cost of those services, not to assure that interventions are effective or wise.
Furthermore, this system underwent extraordinary expansion at the very time where a concurrent expansion in wealth and productivity was also experienced. Thus, this allocation and investment in health care services was not held to the same standards used to assess the wisdom of investment. By insulating the public of the cost, at least in the short term, they were not sensitive to whether this investment was a good investment in their needs and wants. They received a product(s) which appeared to be worth their investment, the size and scope of which they were blissfully unaware.
The lack of investment in coordination of services virtually guarantees that there are huge elements of waste. Because we experienced such dramatic economic growth, the magnitude of that waste could be masked, at least for a while. We are now reaching the point to where that waste cannot be hidden and business as usual cannot go on. However, how does one create effective coordination within a business which has undergone extraordinary growth in both size and scope when so little investment was made in coordination infrastructure?
The issue is not so unique, as noted by Dr. Bowles above. It is foundational to the effective development of any system which delivers basically any product or service to large numbers of people and is integral to any system with depends upon the specialization of labor. This is not a problem, the details of which will yield to proscriptive human efforts and planning, working off some master human plan. The track record of this approach has a perfect batting average, that being perfectly awful and uniform failure.
The title of the subheading immediately prior to the paragraph above in Dr. Bowles book is labeled simply "Getting the rules right". What are those rules which create the correct incentives which allow for complex systems which effectively coordinate human activities? Note that the rules to achieve this are not likely unique to health care environments and we just as likely to gain insights from circumstances divorced from health care delivery than from within.
Given this historical context, the thought that Medicare or some other insurer could fix this problem by creation of a handful of billing codes to pay for "care coordination" is essentially laughable. The fact that a host of disconnected delivery entities has created new coordination issues in their attempts to fix care coordination problems should come not as a surprise.
Saturday, April 11, 2015
Gaming payments and price transparency
Health systems market services which generate margins. They have no choice if they are to survive. All business are based upon this. Even the most minimally astute businessman in health care knows what services are lucrative to deliver. They can not and do not market goods and services which lose them money, even if these services are in great demand and add value to consumers unless they have a philanthropic benefactor which allows them to operate at a loss. Even that cannot go on forever.
What health care services generate substantial margins? That depends upon what can be collected for the service and the cost of delivery. Cost reduction is all of the rage at this point since those who deliver health care services cannot control prices. That is because for most prices for individual services in health care are administratively derived and not subject to market forces. The CPT coding lottery is completely arbitrary and has basically no self correcting capabilities. The price transparency movement is now identifying activities where prices are set too high, resulting in inappropriately extracting value from consumers and payers. However, there is of yet no mechanism for this movement to identify where prices have been set to low and the services are is short supply, have disappeared, or have been so resource starved that the quality of the services has degraded.
There is a certain irony here since the current mantra within health systems is to develop pathways for access as a key principle to capture market share. The problem here is there is little effort to define what the access is to. From those who see this from a macro level and have little understanding of the nuances of clinical care delivery, they are confused as to what the actual deliverables are in health care. The deliverables are not the appointment any more than the essential deliverables is having health insurance. Both insurance and appointments are means to an end, and that end is for the health care delivery system to act at the behest of patients to fix their problems and add value to their lives. The ability to get patients scheduled for an appointment is simply a potential first step in accomplishing those goals. In reality, ready access to the current model may not be the optimal way to address their needs.
As it currently stands, basically the only way for producers to monetize their expertise is to plug patients into inefficient legacy delivery systems which are more geared to extract value from patients than add value. Plug them into a hurried appointment. Work off some checklist of actions defined by PQRS. Collect their copay and bill a third party for the remainder. Maybe listen for a few scant seconds to their complaints. However, whether you meet their needs or not likely has little bearing on getting paid. They got access to something in a timely fashion, not necessarily what they needed or wanted.
Doctors who tinker with different models of payment under the label of concierge practices are often accused of unethical behavior. The reality is they provide services which do not exist in the current system because the price are arbitrarily set below a minimum level of support. There is nothing unethical about offering additional options to patients in a financially transparent way, especially when it creates availability of something of value which would not exist otherwise, that being access to something they really want and/or need.
The real ethical problem comes from a flawed pricing system which creates opportunities to exploit financial arbitrage while adding little value to patients. Imperfect prices set by administrative means will always create these opportunities and humans, being humans, we always exploit them. This is not an approach that can be refined and fixed. Administratively set prices are perhaps useful accounting tools, but they do not and can not transmit essential information about real human needs and priorities. There is no real learning curve here. Any system which depends upon setting prices for goods and services by administrative means can not succeed and will ultimately hugely misallocate resources because flawed human agents will find ways to game the system better and faster than any set of humans can figure out how to stop them.
The simplicity of binaries
Complex human societies have developed over the past 10,000 years. The developments have been gradual but accelerating, especially over the past 500 years. The ability of humans to work together in complex organizations depends upon the existence of complex rules, some legal, but mostly non-legal. These rules evolved and continue to evolve. They are far from perfect. Any framework of rules must get buy in from those who follow them. Rules create boundaries for behavior and those who follow them by definition agree to give up some degrees of freedom of action. The assumption is that whatever is given up must be less than the perceived gains. Otherwise, the rules will not be followed.
The other aspect of rules is their complexity or simplicity. Complex rules require more effort to enforce and apply. Rules tend to become more complex over time as recognition of failure rates of simpler rules becomes evident.The assumption behind this trend is that additional complexity will result in correcting less than optimal outcomes and the tradeoffs involved will not out as a positive. That is not always the case.
The ideal rule depends upon clear distinctions between when actions are required and when they are not. The rule is either activated or it is not. This principle is not limited to scenarios where questions of legal or not legal come into play. Rules are used to govern all sorts of decisions. Where things get complicated is when what has long been appreciated to be governed by rules with unambiguous thresholds are found to be not so clear.
Perhaps my perceptions are not correct, but it appears to me that we are moving to a more complex set of rules over time. I understand that my perceptions are biased and that my reconstructions of the past are likely biased toward a simplicity which never really was there. However, there are some many examples where the choices of the past appear to be some much simpler than they currently are.
When I was a child, we had trash. If something was viewed as something to be disposed, we threw it in a trash can. The big challenge we faced was to change behaviors such that people did not drop trash where they stood or tosh it out of their moving vehicles. We did not have a proliferation choices of where to put materials we wanted to dispose of. We just threw stuff in trash cans and we proud of the fact we did not litter.

Now I am thoroughly confused when I am faced with the proliferation of receptacles. I suffer from disposables anxiety. Am I throwing this in the wrong bin? Do they just get combined and end up in a land fill anyway? Is this some sort of huge scam?
 The proliferation of choices is not limited to trash. Perhaps one of the most fundamental changes which has transpired (and continues to transpire) is the proliferation of choices associated with sex, marriage, civil unions, and partnering. It used to be that you had men and women, and some of those men and women chose to pair up with each other to form families and have children. Some men and women did not pair up and those did not have families. There were some odd circumstances where some men took on multiple wives but this was frowned on and was done only on the fringes of society or in countries where the assumption was they would outgrow this sort of behavior.
The proliferation of choices is not limited to trash. Perhaps one of the most fundamental changes which has transpired (and continues to transpire) is the proliferation of choices associated with sex, marriage, civil unions, and partnering. It used to be that you had men and women, and some of those men and women chose to pair up with each other to form families and have children. Some men and women did not pair up and those did not have families. There were some odd circumstances where some men took on multiple wives but this was frowned on and was done only on the fringes of society or in countries where the assumption was they would outgrow this sort of behavior.
 This simple binary state is gone. There are men who marry men and women who marry women. There are men who end not not wanting to be men and similarly women who decide they do not want to be women, and health care interventions which intervene to create some other state approximating the other sex. These individuals can go on to pair up with other individuals whose sexual orientation or state which can fall somewhere into some continuum, no longer representing the male or female binary (Nature- Sex spectrum).
This simple binary state is gone. There are men who marry men and women who marry women. There are men who end not not wanting to be men and similarly women who decide they do not want to be women, and health care interventions which intervene to create some other state approximating the other sex. These individuals can go on to pair up with other individuals whose sexual orientation or state which can fall somewhere into some continuum, no longer representing the male or female binary (Nature- Sex spectrum).
There are many other examples of where we moved form simple states with few choices to states with multiple choices. Europe had one church for a millenium until the Reformation. The Cold War was about us and them (Soviets). We saw the world in stark terms of good and evil. Now we have a world fragmented into various parties with interlocking and conflicting interests, lead by people who qualify as neither as saints or complete sinners. We confuse legal constraints with the only boundaries defining good and evil.
We can long for some earlier state of the world which was simpler but the reality is it was never so simple. The variations were not appreciated until relatively recently. Perhaps we did not have the time or resources to make much of these distinctions. People in general were too busy simply trying to stay alive. Our predecessors defaulted to simpler constructs, not because they were evil but because they did not have the resources or reserves to accommodate a more nuanced view of the world.
It ultimately goes back to the curse(s) of sedentism. With the passage of time, we have tended to be better at harnessing resources which has created more opportunities to create social and legal complexities which previously could not exist. These complexities allow for the needs and wants of people to differentiate but this differentiation requires more resources and energy and drive us to work harder. They make our lives better but in many senses create a world that is more fragile and structures that are harder to maintain. No single change appears daunting by itself but layered on one another the complexities grow geometrically. Can we understand where additional complexities in social and legal structures go beyond the point(s) of diminishing returns?
The other aspect of rules is their complexity or simplicity. Complex rules require more effort to enforce and apply. Rules tend to become more complex over time as recognition of failure rates of simpler rules becomes evident.The assumption behind this trend is that additional complexity will result in correcting less than optimal outcomes and the tradeoffs involved will not out as a positive. That is not always the case.
The ideal rule depends upon clear distinctions between when actions are required and when they are not. The rule is either activated or it is not. This principle is not limited to scenarios where questions of legal or not legal come into play. Rules are used to govern all sorts of decisions. Where things get complicated is when what has long been appreciated to be governed by rules with unambiguous thresholds are found to be not so clear.
Perhaps my perceptions are not correct, but it appears to me that we are moving to a more complex set of rules over time. I understand that my perceptions are biased and that my reconstructions of the past are likely biased toward a simplicity which never really was there. However, there are some many examples where the choices of the past appear to be some much simpler than they currently are.
When I was a child, we had trash. If something was viewed as something to be disposed, we threw it in a trash can. The big challenge we faced was to change behaviors such that people did not drop trash where they stood or tosh it out of their moving vehicles. We did not have a proliferation choices of where to put materials we wanted to dispose of. We just threw stuff in trash cans and we proud of the fact we did not litter.
Now I am thoroughly confused when I am faced with the proliferation of receptacles. I suffer from disposables anxiety. Am I throwing this in the wrong bin? Do they just get combined and end up in a land fill anyway? Is this some sort of huge scam?
There are many other examples of where we moved form simple states with few choices to states with multiple choices. Europe had one church for a millenium until the Reformation. The Cold War was about us and them (Soviets). We saw the world in stark terms of good and evil. Now we have a world fragmented into various parties with interlocking and conflicting interests, lead by people who qualify as neither as saints or complete sinners. We confuse legal constraints with the only boundaries defining good and evil.
We can long for some earlier state of the world which was simpler but the reality is it was never so simple. The variations were not appreciated until relatively recently. Perhaps we did not have the time or resources to make much of these distinctions. People in general were too busy simply trying to stay alive. Our predecessors defaulted to simpler constructs, not because they were evil but because they did not have the resources or reserves to accommodate a more nuanced view of the world.
It ultimately goes back to the curse(s) of sedentism. With the passage of time, we have tended to be better at harnessing resources which has created more opportunities to create social and legal complexities which previously could not exist. These complexities allow for the needs and wants of people to differentiate but this differentiation requires more resources and energy and drive us to work harder. They make our lives better but in many senses create a world that is more fragile and structures that are harder to maintain. No single change appears daunting by itself but layered on one another the complexities grow geometrically. Can we understand where additional complexities in social and legal structures go beyond the point(s) of diminishing returns?
Sunday, March 1, 2015
The Complacency-Over-reaction Cycle

I came to realize that this sort of cycle, between over-reaction and complacency is characteristic of virtually all human endeavors. When faced with preparing for the future, do we err on the side of doing too much or too little? It depends upon the circumstances we find ourselves in and the memories we have of recent events. No matter how we act at any given time we run the risk, or perhaps the certainty that we are destined to over- or under reaction at some point and we will be wrong. Furthermore, in retrospect we will look stupid, either preparing for some unlikely eventuality or something which happened and appeared to be something we should have anticipated. We will be pilloried by the professional Monday morning quarterbacks.
This phenomena courses through basically every aspect of human existence. Look at the news at the recent vaccination controversy. When I was growing up, vaccinations were not questioned. There were not many of them and those which were available targeted diseases where people had actual memory can contact with. Not take the polio vaccine? You had to be absolutely crazy since there were actual people who were you neighbors who were in iron lungs at some recent point in the past. Fast forward 60 years and we are at the top of the curve, with some parents wondering why we would inflict so many shots on our kids for diseases that NEVER happen. Oh, they do happen....
In foreign affairs, we had the greatest generation which navigated us through WWII and the aggression of Nazi Germany. They witnessed the folly of appeasement and the world war that followed. They also witnessed the over-reaction which resulted in deployment of US troops throughout the world over the next 50 years with less definitive and optimal results. Why did we do all this? What were we thinking? We were thinking that the greatest risk was associated with doing too little but experience has informed us that you perhaps can err in either direction. In the near term, what do we do about the local aggressions of Russia and Putin? Is he the next Hitler or a desperate leader of a marginalized and shrinking country?
We will never get it perfectly right. It is not possible. Furthermore, defining whether we got it right or wrong cannot be defined simply by whether the outcome obtained at any given point in time was what we viewed as ideal. The future has yet to happen and when it arrives we can discern whether we have undershot or overshot our desired goals.

King v. Burwell
Sunday morning is when I take time to read the New York Times. My attention was brought to an Op-ed piece entitled "The phoney legal attack on health care". The title of the piece is erroneous on its face. The case is about the ACA, but this imprecise use of terms appears to be indicative of a broader view of language in general which may provide some insight into the perspective on this specific case. The question is whether imprecise words matter or don't they?
As the editorial board explicitly states:
The Op-ed piece today was pretty much a hit man piece, basically an indignant diatribe predicated on the assumption that this case could simply not be worthy of any merit and if anyone gave it any degree of greater reflection it would be sign that you were simply a moron or some tool of right wing fanaticism (or both). I guess this is what I should expect from the Op-ed page of the Times. It was the Times and it was the Op-Ed page.
Finding a more balanced view became my quest for the morning. It was not particularly easy. However, I did find a piece published in Vox in November 2014 which looked at the arguments which have been presented and will likely be presented (King v. Burwell). In my reading of this there were two key points about the crafting of the legislation which seemed to be important. First, the way this bill became law, through an unconventional budgetary process, meant that it never went to conference committee where inconsistencies between House and Senate versions get cleaned up. The House version pushed a Federal Exchange while the Senate pushed the state exchanges. The original architects of the bill initially acknowledged that the inconsistencies may have been a product of the path to approval. However, they subsequently backtracked on this clam.
The actual language of the statute (the "four words") are pretty unambiguous that subsidies are linked to section 1311, which describes only state-based exchanges. It does not reference section 1321, which sets up the federal exchanges. Whether that was the intent is dependent on who you ask and when you asked them. However, there is no question as to how the actual law is written.There were all sorts of heated discussions regarding other subsidies during the actual debate before passage. There was reportedly no discussion prior to approval of the bill of the state v. federal exchanges and whether subsidies would be available to to specific state run exchanges only.
There has been all sorts of strident speech regarding the Roberts Court and in particular Justice Roberts relating to this case. First, there has been indignation regarding why they chose to even hear this and whether the plaintiffs had standing. Regarding the latter point, I simply don't have sufficient insight to have an informed opinion on the standing issue. Perhaps at the 11th hour the case will evaporate because of lack of standing. It would be convenient and take the Supreme Court off the hook for now. However, assuming the plaintiffs have standing, it would be hard to imagine that the Court could avoid hearing this case.
I can't help but think of Justice Roberts and how he handled the last challenge to the ACA. Through what best can be characterized and legal gymnastics he converted a mandate to purchase a commercial product into a tax, even though the word tax was not written into the legislation. He went to rather extreme lengths to accommodate the intent of the legislative and executive branches of government. I can't help but assume that this case will bring a similar decision. I cannot imagine that the Roberts Court, and particularly Justice Roberts, wants to have the acute consequences of an unconstitutional ruling on their plate. Furthermore, the legal and linguistic twisting involved in this case is no more convoluted that the previous challenge.
I suspect that in the long run this case will have limited impact because the real impact of the ACA will not be through the public exchanges. These will remain at the margins of the health insurance industry. The big story will be the private exchanges which will likely grow at a much faster rate and will dwarf the public exchanges. The ACA stipulated that subsidies and perhaps tax advantages will accrue to those in the public exchanges. With the explosion of private exchanges and movement of employee health insurance of Fortune 500 companies to these exchanges, there is going to be huge pressure to equalize the tax advantages across these products. It may be that this transition is going to continue and accelerate no matter how the case is decided. US business wants to get out of the provision of health insurance benefits.
One of the great ironies of the ACA is it appears to have spurred the development of private health insurance markets which will disrupt our current employer based model and perhaps inject price sanity into what is an otherwise crazy system. I don't suspect that this was not the intent of those who drafted the legislation but perhaps it will be the salvation of the health insurance market. Those on the far left and far right yearn for a collapse of the ACA so they can push to usher in their respective alternative solutions (single payer v. non-governmental). Will the Supreme's be contemplating all of this when they review King v. Burwell? I suspect so but if they are smart, they will decide on the most narrow of terms.
As the editorial board explicitly states:
In the long, tangled history of the debate over the Affordable Care Act, no member of Congress ever indicated a belief that the law would work this way. To the contrary, the law explicitly provides for “quality, affordable health care for all Americans.”Yes, we all know what the intentions of the drafters of the legislation was, but if all that matters is intentions, why go to the bother of drafting anything more? Why not leave it the hands of the legions of well intended people who will ultimately be charged with making the magic happen and we will leave it at their discretion as to how to operationalize this.
The Op-ed piece today was pretty much a hit man piece, basically an indignant diatribe predicated on the assumption that this case could simply not be worthy of any merit and if anyone gave it any degree of greater reflection it would be sign that you were simply a moron or some tool of right wing fanaticism (or both). I guess this is what I should expect from the Op-ed page of the Times. It was the Times and it was the Op-Ed page.
Finding a more balanced view became my quest for the morning. It was not particularly easy. However, I did find a piece published in Vox in November 2014 which looked at the arguments which have been presented and will likely be presented (King v. Burwell). In my reading of this there were two key points about the crafting of the legislation which seemed to be important. First, the way this bill became law, through an unconventional budgetary process, meant that it never went to conference committee where inconsistencies between House and Senate versions get cleaned up. The House version pushed a Federal Exchange while the Senate pushed the state exchanges. The original architects of the bill initially acknowledged that the inconsistencies may have been a product of the path to approval. However, they subsequently backtracked on this clam.
The actual language of the statute (the "four words") are pretty unambiguous that subsidies are linked to section 1311, which describes only state-based exchanges. It does not reference section 1321, which sets up the federal exchanges. Whether that was the intent is dependent on who you ask and when you asked them. However, there is no question as to how the actual law is written.There were all sorts of heated discussions regarding other subsidies during the actual debate before passage. There was reportedly no discussion prior to approval of the bill of the state v. federal exchanges and whether subsidies would be available to to specific state run exchanges only.
There has been all sorts of strident speech regarding the Roberts Court and in particular Justice Roberts relating to this case. First, there has been indignation regarding why they chose to even hear this and whether the plaintiffs had standing. Regarding the latter point, I simply don't have sufficient insight to have an informed opinion on the standing issue. Perhaps at the 11th hour the case will evaporate because of lack of standing. It would be convenient and take the Supreme Court off the hook for now. However, assuming the plaintiffs have standing, it would be hard to imagine that the Court could avoid hearing this case.
I can't help but think of Justice Roberts and how he handled the last challenge to the ACA. Through what best can be characterized and legal gymnastics he converted a mandate to purchase a commercial product into a tax, even though the word tax was not written into the legislation. He went to rather extreme lengths to accommodate the intent of the legislative and executive branches of government. I can't help but assume that this case will bring a similar decision. I cannot imagine that the Roberts Court, and particularly Justice Roberts, wants to have the acute consequences of an unconstitutional ruling on their plate. Furthermore, the legal and linguistic twisting involved in this case is no more convoluted that the previous challenge.
I suspect that in the long run this case will have limited impact because the real impact of the ACA will not be through the public exchanges. These will remain at the margins of the health insurance industry. The big story will be the private exchanges which will likely grow at a much faster rate and will dwarf the public exchanges. The ACA stipulated that subsidies and perhaps tax advantages will accrue to those in the public exchanges. With the explosion of private exchanges and movement of employee health insurance of Fortune 500 companies to these exchanges, there is going to be huge pressure to equalize the tax advantages across these products. It may be that this transition is going to continue and accelerate no matter how the case is decided. US business wants to get out of the provision of health insurance benefits.
One of the great ironies of the ACA is it appears to have spurred the development of private health insurance markets which will disrupt our current employer based model and perhaps inject price sanity into what is an otherwise crazy system. I don't suspect that this was not the intent of those who drafted the legislation but perhaps it will be the salvation of the health insurance market. Those on the far left and far right yearn for a collapse of the ACA so they can push to usher in their respective alternative solutions (single payer v. non-governmental). Will the Supreme's be contemplating all of this when they review King v. Burwell? I suspect so but if they are smart, they will decide on the most narrow of terms.
Sunday, February 15, 2015
The useful functions of vaccine deniers
I was born into a unique generation in the history of mankind. My generation in the US was the first generation which grew up with almost no fears of infectious disease. The polio epidemic, which raged in its worst form immediately prior to my birth, was reigned in by the miracle of the Salk and Sabin vaccines. The antibiotic era began immediately before and one remarkable agent after another was brought to market in my childhood. While there were a number of childhood diseases which I had to weather (measles, mumps, and varicella), the terrifying scourges were for the most part vanquished.
For the next few decades, we became increasingly complacent about vaccination and these diseases which became of interest mostly because of historical interest. The memory of polio, whooping cough, diphtheria, measles, and chickpox became increasingly distant. Yes, if you cut yourself and appeared for acute care you received a tetanus shot, almost like some sort of religious ritual. Throw some salt over your left shoulder or say gesundheit when someone sneezes or coughs. No one gets those diseases anymore, do they?
The general public had increasingly fewer and fewer reference points to judge the need for vaccinations. The generations which experienced infantile paralysis or other less harrowing childhood diseases are dying off and the reality of such diseases have become nothing but distant echos. It is not at all surprising that skeptical voices have emerged. While I believe that these voices as relating to vaccine issues are barking up the wrong tree, I also believe it is important to cultivate skeptical voices. Expert classes tend to become increasingly insulated and self serving over time and the skeptical voices are important to provide feedback from broader, non-expert audiences who ultimately the experts must answer to.
An experiment has been done. The subjects unfortunately were the children of parents who were skeptical of the value of the measles vaccine. The results were the re-emergence of isolated pockets measles. The feedback is if you don't vaccinate your children they are at higher risk of getting sick. The news has been widely broadcasted. There is value in this. One could argue that children should not suffer the consequences of bad judgements of their parents. That however can never be avoided and the risks of striving to use the power of the state to reach those utopian goals will result in much more harm than could ever be perpetrated by the isolated bad judgement of selected parents.
Those of us who make bad decisions (which is all of us sometime) can serve useful functions when the unfortunate circumstances which befall us become apparent to those around us. We can but should not insulate people from the consequences of their bad decisions. Bad outcomes provide the feedback that tells us that we should not have done specific things. In the case of the parents who make unwise decisions regarding vaccination, we should not be timid about pointing out the errors. However, we also should not deploy tyrannical approaches in an attempt to reign in all sorts of bad judgements. It won't work and it runs the real risk of putting power into the hands of people and entities which want to run peoples lives.
I envision there will always be an ebb and flow when it comes to compliance with vaccination. As we are more successful with vaccine adoption the rates of disease will go down, but over the time the rates of complacency will go up, resulting in lower vaccination rates and resurgence of disease. It should be self correcting except for places such the Swat Valley. It may be unfortunate but the voices of science cannot fight complacency nearly as effectively as the predictable resurgence of disease in a complacent population.
For the next few decades, we became increasingly complacent about vaccination and these diseases which became of interest mostly because of historical interest. The memory of polio, whooping cough, diphtheria, measles, and chickpox became increasingly distant. Yes, if you cut yourself and appeared for acute care you received a tetanus shot, almost like some sort of religious ritual. Throw some salt over your left shoulder or say gesundheit when someone sneezes or coughs. No one gets those diseases anymore, do they?
The general public had increasingly fewer and fewer reference points to judge the need for vaccinations. The generations which experienced infantile paralysis or other less harrowing childhood diseases are dying off and the reality of such diseases have become nothing but distant echos. It is not at all surprising that skeptical voices have emerged. While I believe that these voices as relating to vaccine issues are barking up the wrong tree, I also believe it is important to cultivate skeptical voices. Expert classes tend to become increasingly insulated and self serving over time and the skeptical voices are important to provide feedback from broader, non-expert audiences who ultimately the experts must answer to.
An experiment has been done. The subjects unfortunately were the children of parents who were skeptical of the value of the measles vaccine. The results were the re-emergence of isolated pockets measles. The feedback is if you don't vaccinate your children they are at higher risk of getting sick. The news has been widely broadcasted. There is value in this. One could argue that children should not suffer the consequences of bad judgements of their parents. That however can never be avoided and the risks of striving to use the power of the state to reach those utopian goals will result in much more harm than could ever be perpetrated by the isolated bad judgement of selected parents.
Those of us who make bad decisions (which is all of us sometime) can serve useful functions when the unfortunate circumstances which befall us become apparent to those around us. We can but should not insulate people from the consequences of their bad decisions. Bad outcomes provide the feedback that tells us that we should not have done specific things. In the case of the parents who make unwise decisions regarding vaccination, we should not be timid about pointing out the errors. However, we also should not deploy tyrannical approaches in an attempt to reign in all sorts of bad judgements. It won't work and it runs the real risk of putting power into the hands of people and entities which want to run peoples lives.
I envision there will always be an ebb and flow when it comes to compliance with vaccination. As we are more successful with vaccine adoption the rates of disease will go down, but over the time the rates of complacency will go up, resulting in lower vaccination rates and resurgence of disease. It should be self correcting except for places such the Swat Valley. It may be unfortunate but the voices of science cannot fight complacency nearly as effectively as the predictable resurgence of disease in a complacent population.
Saturday, January 31, 2015
Title IX hysteria
I am supposed to live in an academic world where we value critical thinking skills. However, I have a growing concern about the clash between the skepticism required for reflective thought and the academic embrace of advocacy driven "scholarship". Nowhere is this more apparent than the recent injection of Title IX fever into college campuses, driven by a zealotus Federal bureaucracy.
Stories about an epidemic of sexual violence on college campuses have peppered the new outlets this past year. There is an industry out there looking for growth opportunities in this realm and some within the industry do not appear to be constrained by any desire to operate driven by fact or truth. One of the more egregious examples centered around the story that came out of the University of Virginia which was reported in Rolling Stone magazine. Whether it represented a complete or partial hoax is not entirely clear but there is no question that many if not most of the story's details were completely implausible.
However, recent initiatives driven by the Federal government have been driven by the impression that there is a huge problem on college campuses which can only be addressed by imposition of new rules driven by the Feds. The leverage they have is through the federalization of higher education funding which allows them to hold virtually all colleges hostage to whatever bureaucratic whim is fashionable in Washington DC.
The data which appears to justify such an overarching reach by the Feds has been called into question. There is a figure thrown around of 1 in 5 women as being a victim of sexual assault. This figure comes from a 2007 survey from the DOJ. Shortly after this study was reported in a story in Slate, a much larger survey done the Justice Department Bureau of Justice Statistics found a rate of 0.6%, substantially lower than the 20% figure previously reported. The former study involved two unnamed public universities while the latter surveyed 90,000 households and 160,000 individuals encompassing a much broader swath of students.
Imagine my surprise when I received an email from my Title IX compliance officer ordering me and all of my colleagues to take a course regarding sexual violence on campus. When the Feds say jump, we say, how high? This enterprise comes directly Whitehouse.gov(Campus assault). Consistent with his activist roots, President Obama does not appear to be troubled by citation of the questionable 1 in 5 statistic. Advocacy is generally not effective when accompanied by any sort of self reflection of self skepticism.
To further my surprise, when I logged into the learning module to "educate" me and bring my into compliance with Title IX training, what statistic was placed immediately front and center? The same 1 in 5 number . I went online and did an internet search for Title IX training materials and what did I find in these as well? The same statistic. If I were grading a presentation by one of my students and I found that they had chosen to highlight a single study which was flawed and ignore information from more robust studies, they would get a failing grade.
However, I soldiered through the roughly one hour course, clicking through a series of scenarios and questions, picking the "right" answers. The scenarios were ambiguous and the exercise resembled an indoctrination more than an educational activity. The scenarios dealt with perhaps the most complex, difficult, and ambiguous contexts of human interactions; sexual encounters and alcohol. Each one perhaps could serve as a starting point for thoughtful discussions which might go on for an entire semester and PhD ethics thesis. However, in this training session and in final exam, I was called upon to pick the one and only right answer. I was being put on notice. No input was asked of me and there is essentially no mechanism where I can provide feedback on this. I understand. No feedback is wanted.
More than two dozen luminaries within the Harvard Law School have come out with a statement protesting their University's new rules regarding title IX. They have the standing and legal scholarship to do so. I do not. I know in my heart that continuation in the direction will end badly for most of us. The same people who vetted the online training courses have already shown they are not objective and will not let disparate opinions and data get in the way of furthering their particular lines of advocacy. Yet, they are ones who will be put in charge of adjudicating Title IX issues on campus. They will direct investigations, oversee tribunals, and render decisions.
Colleges and universities are in a similar position to me. They are not in a position to bargain with the Feds. To much money is at stake and there is no foreseeable pathway to success that can be envisioned by confrontation. The risk of losing the income stream driven by fully federalized tuition loans, federal research grants, and federal health care dollars. Monopsony in business has its downside.
Human interactions are complex. Human sexual relations are the most complex subset of interactions within these interactions. I will be the first to admit we have not yet worked out all the rules on this realm, despite working on them for thousands of years. What the Federal government is trying to do is to create some sort of separate formal review and response structure on college campuses based upon the idea that an urgent need exists. That perceived need is likely based faulty data. The solutions proposed ignore basic concepts of due process and protection of the accused. It seems like such a bad idea. However, very few are in a position to raise our concerns.
Stories about an epidemic of sexual violence on college campuses have peppered the new outlets this past year. There is an industry out there looking for growth opportunities in this realm and some within the industry do not appear to be constrained by any desire to operate driven by fact or truth. One of the more egregious examples centered around the story that came out of the University of Virginia which was reported in Rolling Stone magazine. Whether it represented a complete or partial hoax is not entirely clear but there is no question that many if not most of the story's details were completely implausible.
However, recent initiatives driven by the Federal government have been driven by the impression that there is a huge problem on college campuses which can only be addressed by imposition of new rules driven by the Feds. The leverage they have is through the federalization of higher education funding which allows them to hold virtually all colleges hostage to whatever bureaucratic whim is fashionable in Washington DC.
The data which appears to justify such an overarching reach by the Feds has been called into question. There is a figure thrown around of 1 in 5 women as being a victim of sexual assault. This figure comes from a 2007 survey from the DOJ. Shortly after this study was reported in a story in Slate, a much larger survey done the Justice Department Bureau of Justice Statistics found a rate of 0.6%, substantially lower than the 20% figure previously reported. The former study involved two unnamed public universities while the latter surveyed 90,000 households and 160,000 individuals encompassing a much broader swath of students.
Imagine my surprise when I received an email from my Title IX compliance officer ordering me and all of my colleagues to take a course regarding sexual violence on campus. When the Feds say jump, we say, how high? This enterprise comes directly Whitehouse.gov(Campus assault). Consistent with his activist roots, President Obama does not appear to be troubled by citation of the questionable 1 in 5 statistic. Advocacy is generally not effective when accompanied by any sort of self reflection of self skepticism.
To further my surprise, when I logged into the learning module to "educate" me and bring my into compliance with Title IX training, what statistic was placed immediately front and center? The same 1 in 5 number . I went online and did an internet search for Title IX training materials and what did I find in these as well? The same statistic. If I were grading a presentation by one of my students and I found that they had chosen to highlight a single study which was flawed and ignore information from more robust studies, they would get a failing grade.
However, I soldiered through the roughly one hour course, clicking through a series of scenarios and questions, picking the "right" answers. The scenarios were ambiguous and the exercise resembled an indoctrination more than an educational activity. The scenarios dealt with perhaps the most complex, difficult, and ambiguous contexts of human interactions; sexual encounters and alcohol. Each one perhaps could serve as a starting point for thoughtful discussions which might go on for an entire semester and PhD ethics thesis. However, in this training session and in final exam, I was called upon to pick the one and only right answer. I was being put on notice. No input was asked of me and there is essentially no mechanism where I can provide feedback on this. I understand. No feedback is wanted.
More than two dozen luminaries within the Harvard Law School have come out with a statement protesting their University's new rules regarding title IX. They have the standing and legal scholarship to do so. I do not. I know in my heart that continuation in the direction will end badly for most of us. The same people who vetted the online training courses have already shown they are not objective and will not let disparate opinions and data get in the way of furthering their particular lines of advocacy. Yet, they are ones who will be put in charge of adjudicating Title IX issues on campus. They will direct investigations, oversee tribunals, and render decisions.
Colleges and universities are in a similar position to me. They are not in a position to bargain with the Feds. To much money is at stake and there is no foreseeable pathway to success that can be envisioned by confrontation. The risk of losing the income stream driven by fully federalized tuition loans, federal research grants, and federal health care dollars. Monopsony in business has its downside.
Human interactions are complex. Human sexual relations are the most complex subset of interactions within these interactions. I will be the first to admit we have not yet worked out all the rules on this realm, despite working on them for thousands of years. What the Federal government is trying to do is to create some sort of separate formal review and response structure on college campuses based upon the idea that an urgent need exists. That perceived need is likely based faulty data. The solutions proposed ignore basic concepts of due process and protection of the accused. It seems like such a bad idea. However, very few are in a position to raise our concerns.
Sunday, January 11, 2015
The world is a work in progress
I saw the movie "Imitation game" last night. It is about Alan Turing and his efforts to break the Nazi Enigma code in WWII. It was simply a tragedy of epic proportions that the world lost him at the young age of 41, after he was convicted of solicitation of homosexual sex and forced under court order to take medications which chemically castrated him. Britain at that time considered homosexuality a crime. He committed suicide in the year of my birth.
I remember my first exposure to homosexuals when I was in college. There were a cadre of effeminate men which I did not recall from my high school experience. I may have simply been unaware of this cohort earlier in my schooling. I was rather young and not tuned into these issues. The thought of being attractive to other men was completely alien to my preferences. It had simply never even occurred to me that could be an option at that point in my life. However, I could not consider that homosexuality was a crime at that time, although I think anti-sodomy laws were on the books. They may still be on the books.
This particular cohort at college was almost universally ridiculed among those who I associated with. At that point in time I did not view this with any sort of moral dimension. I perceived this cohort simply as something very strange. I never acted in a way to personally ridicule anyone for their apparent homosexuality. However, I also did not take any action to step up in defense of anyone or call anyone out on their anti-homosexual actions. Knowing what I know now, I could have been more heroic in coming to the defense of those who were identified as being homosexual men. I was simply struggling to find my way at that time.
Roll the clock forward more than forty years. The world is a very different place. I am a very different person or at least I have a very different perspective on my world. I have had the experience of meeting literally thousands of people, both personally and professionally. I have come to realize just how remarkably diverse people are in terms of motivation, responses to incentives, preferences, talents, virtues, and vices. I have come to realize that David Hume was correct in terms of "reason being a slave to passion" and that many if not most of our passions are beyond our choice.
The world is a simpler place when the choices are binary. It makes for simpler law and simpler choices in the personal realm. However, the world is generally not black and white in terms of our choices. The growing acceptance of homosexuality and what could viewed in historical terms as atypical sexual practices is a product of recent decades in a small subset of human cultures. It may be viewed as part of a longer term trend in human societies of greater acceptance of diversity in general. It is my belief that this is a consequence of greater human affluence in general.
Cultures which live on the edge have less reserves to play with. Mistakes which affect the ability to feed or defend themselves literally can represent existential threats. An almost universal characteristic of human societies has been to hold anyone or anything that is different with great suspicion. Call it the stranger heuristic. The default response to strangers was violence. The default response to almost everything was violence. In a zero sum world which was the world until that past 500 years, that response may have had some survival advantages.
I have had the opportunity to live and experience a world where we can tolerate outliers. In fact, our world may benefit from harnessing the talents of those who we might view initially as strange. It is not as if we cannot define certain actions as unacceptable. We need to re-examine what we might have viewed as outside the bounds as acceptable. We will not all agree on what is acceptable or not acceptable but we should be very careful about using the coercive power of the state to enforce anything but the most egregious and unacceptable actions. On the flip side, we should also allow leeway to individuals to define their own comfort zones, using social sanctions to provide feedback to those within voluntary social networks. The world is a work in progress.
I remember my first exposure to homosexuals when I was in college. There were a cadre of effeminate men which I did not recall from my high school experience. I may have simply been unaware of this cohort earlier in my schooling. I was rather young and not tuned into these issues. The thought of being attractive to other men was completely alien to my preferences. It had simply never even occurred to me that could be an option at that point in my life. However, I could not consider that homosexuality was a crime at that time, although I think anti-sodomy laws were on the books. They may still be on the books.
This particular cohort at college was almost universally ridiculed among those who I associated with. At that point in time I did not view this with any sort of moral dimension. I perceived this cohort simply as something very strange. I never acted in a way to personally ridicule anyone for their apparent homosexuality. However, I also did not take any action to step up in defense of anyone or call anyone out on their anti-homosexual actions. Knowing what I know now, I could have been more heroic in coming to the defense of those who were identified as being homosexual men. I was simply struggling to find my way at that time.
Roll the clock forward more than forty years. The world is a very different place. I am a very different person or at least I have a very different perspective on my world. I have had the experience of meeting literally thousands of people, both personally and professionally. I have come to realize just how remarkably diverse people are in terms of motivation, responses to incentives, preferences, talents, virtues, and vices. I have come to realize that David Hume was correct in terms of "reason being a slave to passion" and that many if not most of our passions are beyond our choice.
The world is a simpler place when the choices are binary. It makes for simpler law and simpler choices in the personal realm. However, the world is generally not black and white in terms of our choices. The growing acceptance of homosexuality and what could viewed in historical terms as atypical sexual practices is a product of recent decades in a small subset of human cultures. It may be viewed as part of a longer term trend in human societies of greater acceptance of diversity in general. It is my belief that this is a consequence of greater human affluence in general.
Cultures which live on the edge have less reserves to play with. Mistakes which affect the ability to feed or defend themselves literally can represent existential threats. An almost universal characteristic of human societies has been to hold anyone or anything that is different with great suspicion. Call it the stranger heuristic. The default response to strangers was violence. The default response to almost everything was violence. In a zero sum world which was the world until that past 500 years, that response may have had some survival advantages.
I have had the opportunity to live and experience a world where we can tolerate outliers. In fact, our world may benefit from harnessing the talents of those who we might view initially as strange. It is not as if we cannot define certain actions as unacceptable. We need to re-examine what we might have viewed as outside the bounds as acceptable. We will not all agree on what is acceptable or not acceptable but we should be very careful about using the coercive power of the state to enforce anything but the most egregious and unacceptable actions. On the flip side, we should also allow leeway to individuals to define their own comfort zones, using social sanctions to provide feedback to those within voluntary social networks. The world is a work in progress.
Saturday, January 10, 2015
Needing an industrial revolution in healthcare
I recently finished a Teaching Company course on the Industrial Revolution, taught by Dr. Patrick Allitt. In this course he detailed the development of industrialization of manufacturing over the course of almost 500 years. It is a remarkable story of human ingenuity, technological progress, and extraordinary impact on the human condition. He presents a story of a world not so long ago where human existence was precarious because the tools and systems in place to meet human needs were rudimentary. The remarkable development of industrial technologies in conjunction with effective approaches to motivate and coordinate human activity resulted in a complete transformation of human existence where these tools were deployed.

The progress did not take place in a straight line. There were failures and the achievements made were the product of much tinkering and some planning. The exact outcomes were not necessarily predictable but the themes in retrospect were recurrent. At each step of the way, huge breakthroughs happened when tools were developed that freed humans from manual tasks and automated activities. These breakthroughs were almost always very disruptive of selected industries and populations but the net effects for the broader population were hugely positive. People got more to eat at lower prices as well as better living and working conditions.
Another aspect of this evolution was the ability of the industrial revolution to deliver not only more, but more at a lower price and higher quality. Nowhere is this more evident than in the 20th century where we observed an explosion of increasingly sophisticated consumer goods where after particular product introductions prices would tumble while simultaneously the functionality and quality increased. This includes computers, home appliances, and automobiles. What drove this remarkable expansion of high quality plenty was a combination of science, breakthroughs in human organization, and information systems which could track key elements of cost and quality.

Dr. Allitt tracks all of these elements going back to their origins, which he tracks back to the building and operation of large ships in England. What does this have to do with medicine and biomedical research? Simply that the health care delivery and research relating to health care benefits from the same tools which made the industrial revolution possible. The holy grail for basically any human activity is to get more out of any particular inputs in terms of making human lives better. It has been well documented that, unlike the productivity gains associated with virtually all commercial activities in the US since WWII, health care has shown essentially no productivity gains. As noted by by Kochner, et all in the NEJM (N Engl J Med 2011; 365:1370-1372October 13, 2011DOI: 10.1056/NEJMp1109649):
The story in biomedical research is perhaps a bit more nuanced. Biomedical research has revolutionized diagnostics and therapeutics but we are facing issues of diminishing returns. The antibiotic and vaccine revolution deployed in the early to mid 20th century made huge impacts at very modest cost. Arguably the returns of these endeavors dwarfed the costs of development and deployment. We are at a different point now where the cost of new drugs to treat chronic diseases is simply off the charts. Every new decade moves the decimal place over one place. Furthermore, the deliverables for individual researchers is not necessarily something that has an impact on people in the near term. The funding system values a different sort of productivity based upon publications. The explosion of scientific publishing has until recently, not been accompanied by any real change in the mechanics of vetting and review and the problem which has arisen is one of quality control.
However, funding agencies have attempted to develop models to oversee quality and independent entities such as Retraction Watch (http://retractionwatch.com/) have stepped up to inject quality control in the process not adequately addressed with peer review. Not surprisingly there has been an explosion of paper retractions as well as exposees revealing major issues with reproducibility (Nature article). This is very disturbing because what separates science from magic and alchemy is the ability to reproduce results.
What all of these contemporary processes have in common is they are very dependent upon human beings using manual processes and judgement requiring much subjectivity to do their jobs. Furthermore, the products of these efforts cannot be readily and consistently assessed for quality. As long as these remains the case in health care delivery and biomedical research, it will be hard to reap the sort of gains from investment in these sectors when compared to investments made in areas where productivity and quality can be assessed more robustly.
The progress did not take place in a straight line. There were failures and the achievements made were the product of much tinkering and some planning. The exact outcomes were not necessarily predictable but the themes in retrospect were recurrent. At each step of the way, huge breakthroughs happened when tools were developed that freed humans from manual tasks and automated activities. These breakthroughs were almost always very disruptive of selected industries and populations but the net effects for the broader population were hugely positive. People got more to eat at lower prices as well as better living and working conditions.
Another aspect of this evolution was the ability of the industrial revolution to deliver not only more, but more at a lower price and higher quality. Nowhere is this more evident than in the 20th century where we observed an explosion of increasingly sophisticated consumer goods where after particular product introductions prices would tumble while simultaneously the functionality and quality increased. This includes computers, home appliances, and automobiles. What drove this remarkable expansion of high quality plenty was a combination of science, breakthroughs in human organization, and information systems which could track key elements of cost and quality.
Dr. Allitt tracks all of these elements going back to their origins, which he tracks back to the building and operation of large ships in England. What does this have to do with medicine and biomedical research? Simply that the health care delivery and research relating to health care benefits from the same tools which made the industrial revolution possible. The holy grail for basically any human activity is to get more out of any particular inputs in terms of making human lives better. It has been well documented that, unlike the productivity gains associated with virtually all commercial activities in the US since WWII, health care has shown essentially no productivity gains. As noted by by Kochner, et all in the NEJM (N Engl J Med 2011; 365:1370-1372October 13, 2011DOI: 10.1056/NEJMp1109649):
Of the $2.6 trillion spent in 2010 on health care in the United States, 56% consisted of wages for health care workers. Labor is by far the largest category of expense: health care, as it is designed and delivered today, is very labor-intensive. The 16.4 million U.S. health care employees represented 11.8% of the total employed labor force in 2010. Yet unlike virtually all other sectors of the U.S. economy, health care has experienced no gains over the past 20 years in labor productivity, defined as output per worker (in health care, the “output” is the volume of activity — including all encounters, tests, treatments, and surgeries — per unit of cost). Although it is possible that some gains in quality have been achieved that are not reflected in productivity gains, it's striking that health care is not experiencing anything near the gains achieved in other sectors. At the same time, health care labor is becoming more expensive more quickly than other types of labor. Even through the recession, when wages fell in other sectors, health care wages grew at a compounded annual rate of 3.4% from 2005 to 2010.In addition, it is very difficult to demonstrate gains in quality as well. I contend that these two shortfalls are in fact related to the inadequacy in information systems used in health care. When you can't reliably track things, you end up wasting resources and generating poor quality products.
The story in biomedical research is perhaps a bit more nuanced. Biomedical research has revolutionized diagnostics and therapeutics but we are facing issues of diminishing returns. The antibiotic and vaccine revolution deployed in the early to mid 20th century made huge impacts at very modest cost. Arguably the returns of these endeavors dwarfed the costs of development and deployment. We are at a different point now where the cost of new drugs to treat chronic diseases is simply off the charts. Every new decade moves the decimal place over one place. Furthermore, the deliverables for individual researchers is not necessarily something that has an impact on people in the near term. The funding system values a different sort of productivity based upon publications. The explosion of scientific publishing has until recently, not been accompanied by any real change in the mechanics of vetting and review and the problem which has arisen is one of quality control.
However, funding agencies have attempted to develop models to oversee quality and independent entities such as Retraction Watch (http://retractionwatch.com/) have stepped up to inject quality control in the process not adequately addressed with peer review. Not surprisingly there has been an explosion of paper retractions as well as exposees revealing major issues with reproducibility (Nature article). This is very disturbing because what separates science from magic and alchemy is the ability to reproduce results.
What all of these contemporary processes have in common is they are very dependent upon human beings using manual processes and judgement requiring much subjectivity to do their jobs. Furthermore, the products of these efforts cannot be readily and consistently assessed for quality. As long as these remains the case in health care delivery and biomedical research, it will be hard to reap the sort of gains from investment in these sectors when compared to investments made in areas where productivity and quality can be assessed more robustly.
Subscribe to:
Posts (Atom)