
http://online.wsj.com/article/SB10001424052748704851204576034332420051722.html.
http://online.wsj.com/article/SB10001424052748704457604576011382824069032.html.
The comments which followed the article fall into the usual finger pointing mode... inept government, unethical providers, FMG's, inevitability due to human nature, etc. I am reminded of the mantra of the healthcare safety movement that unfortunate results are often the result of poor system design which predictably generate undesirable outcomes.
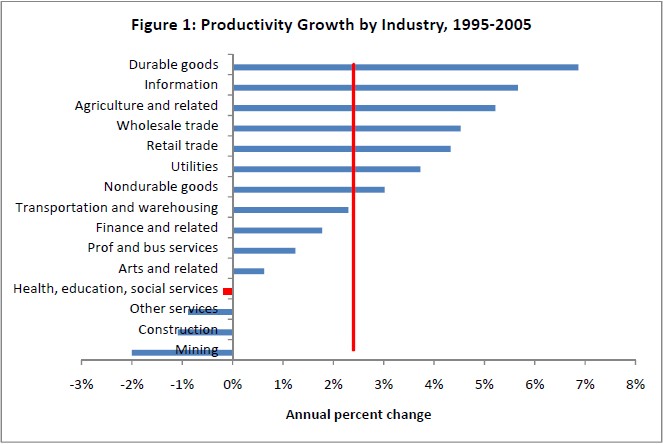
Let us look at the story described in the WSJ article. A particular high profile doc in south Florida aggressively bills Medicare for physical therapy services to the tune of millions of dollars. Our immediate response is this is unscrupulous and he has been gaming the system. This is likely a correct conclusion but perhaps a deeper analysis is warranted. What part of his activities were undesirable? Is it the fact that he was able to project his expertise and services to large numbers of patients? In other realms of business that is viewed rather positively. In fact, one of the major criticisms of the health care industry has been the lack of productivity gains over the past 40 years.
http://theincidentaleconomist.com/wordpress/the-health-care-productivity-problem/
Was he claiming to deliver services when the work was delegated to some other person? That is a possibility but again, where is the harm if the patient actually received and benefited from the service. Is that not gain sharing? Licensing requirements may have been violated but if the patients received the service and benefited from this (and were not harmed), it is more likely that the licensing requirements are serving the provider guilds more than the patients. Delegation to less expensive providers and movement to rules based delivery systems drive productivity gains. If we use volume as a criteria to identify fraud, we will be inadvertently targeting the very entrepreneurial innovators who can lead us to productivity gains.
Was he actually delivering value to the patients that he served? We have absolutely no idea. Here lies the problem. We have deployed a payment system which divorces the payment from the actual delivery of value. This actually is built into the system at multiple levels. First, the actual level of payment for services is set administratively and it is set to a one size fits all. No matter how valuable the service is to any given patient the value to the provider to deliver the service is the same. The pricing system is devoid of differentials to prioritize who should actually receive the service. On one side, this prevents those from who value the service most highly from being priority customers and on the other side, it creates a perverse incentive to deploy the service to even those who will derive little or no value from it.
Even if there was some sort of price differential based upon actual value to the recipient, the insulation of those actually receiving the service from the entities paying for it means there is an almost total loss of discipline in the process. In the case of the physical therapy sessions billed by this Florida physician, which patients are not going to like getting back rubs that they do not pay for. I suspect that if Medicare were to survey the patients who received the services to determine whether they believed they were the victims of fraud, they would likely find very few who believed they had been victims. Even the ones who received no services at all, why should they care? They likely received no bills either. Design a system like this and what do you expect? While at the onset most participants will stay within the lines, it only takes a few "gamers" to discover and exploit the weaknesses. The rest of the world will follow them when they are cautioned not to leave money on the table redefining the bounds of decency as they do so.
The fundamental flaw is the financial triangle. Two way exchanges are not nearly as open to rampant fraud because those who pay are the ones who receive the service. No service, no payment. No payment, no service. The three way is never desirable and even more so in a realm where there are not ready checks and balances. Transaction one is to send the money to some agent whose primary desire is to hold on to the cash. Transaction two is some sort of medical service delivered by an agent who has a motivation to do as many things as possible and convince the recipient of those services that they are necessary and valuable. Transaction three is the claim of the health care provider on some share of the cash accumulated by the payer from transaction one. Distantly linked to the previous transactions are the purchase of health insurance which is temporally divorced from the actual delivery of services and only opaquely linked in terms of cost and use. There are essentially no immediate or delayed rewards for anything resembling good citizenship. Those who come out ahead financially are ones who game early and often. The difference between "legitimate" gaming and fraud is blurring to start with and morphs constantly over time.
The point is there will always be people who game whatever system that exists. Once the pioneers demonstrate that pushing the envelope creates financial windfalls, even those with less entrepreneurial spirit follow their leads. In the marketplace of a price coordinated economy where those who receive the service actually pay for it, fraud exists but it is hard for it to grow to such proportions. People who pay with their own resources are much more prudent in terms of spending. Furthermore, the more people who exploit particular avenues, the greater the availability of particular services and the more the price falls. Systems such as Medicare have few feedback loops to identify real value and have no real time price signals. Supply has little relation to demand. For Medicare, price is simply an accounting device devoid of the ability to coordinate human activity within any meaningful time frame. Providers respond to price by doing more of what drives their margins irrespective of what value is brought to patients.
The talent available looking for points of weakness will always outstrip the ability to detect and respond effectively to fraud. No matter how robust the engineering appears to be, it will always be flawed since it is based upon a foundation which cannot support it.
No comments:
Post a Comment