
I have remarkably fortunate in terms of illness in my family. My children have experienced a variety of health problems, some of which required hospitalization. However, my wife and I are medical professionals and we have know how on how to deal with the medical delivery system. We knew when specific issues needed to be dealt with immediately and where to go to effectively solve specific problems.
Both of my parents have been remarkably healthy until very recently, which I have viewed as a remarkable blessing. Over the past month, my father has developed some new health issues and each time my parents have health problems or encounters with the health care system, I learn I have some new blindspot when it comes to appreciating the health care system. I have come to realize is that minor health concerns which force one to interact with elements of the health care delivery system as like small dress rehearsals for when something major comes along. Without these dress rehearsals, even the most educated and together people are ill prepared to deal with new and major health issues.
My medical education and even more so my experience in practice has taught me about effective approaches to managing illness (even my own) and the capabilities and limits of current medical care. The question is, how much of this knowledge base is part of an ordinary education? The answer is almost none. It made me think back upon my own education prior to my dive into medicine. I recall my first exposure to human health issues, that being health class in middle school and high school. It was an absolute joke focusing (rather ineffectively) on sex ed, sexually transmitted diseases,drugs and alcohol. While these are rather high stakes issues and I do not want to discount any importance of any effective approaches to deal with this, two obvious observations remain.
First, the courses were a joke and completely ineffective. Those who taught them tended to be poorly prepared and the brunt of jokes. From what my own grown children tell me, there has been little change since I was growing up. Second, the range of experiences I have had dealing with health issues both personally and professionally had focused on a set of experiences which is completely distinct from what was highlighted in my health classes. What perhaps is most striking is the complete lack of any practical knowledge regarding how to navigate the health care delivery system when an individual or family member is ill.
What struck me about my father's recent health issues is how completely unaware my parents were about how to deal with basic health issues. They had no notion of what constitutes urgency, what issues they should be concerned about and which ones were less ominous, and where they should go to have specific issues addressed. They are both very intelligent and well read and have a lifetime of experience in other realms. It is nothing short of remarkable that such highly educated people can have such a huge blind spot.
Perhaps it is not that surprising since our present education system is rather biased away from practical knowledge. Health education professionals are rewarded to focus on high profile and titillating public health targets such as sexually transmitted diseases and obesity despite the apparent futility of such quests. It is my opinion that the time would be better spent educating people about perhaps more mundane but very practical aspects of health and health care.
This could include simple rules based approaches to ubiquitous illnesses. Virtually everyone can expect to develop URI's, a myriad of GI illnesses, urinary tract infections, yeast infections, dermatitis, wheezing, lacerations and abrasion, sprains and possible breaks, and soft tissue injuries. All of these common scenarios have rules based protocols which should not be viewed as trade secrets. It is nothing short of bizarre that students complete a college education and have no clue as what to do when they (or a family member such as a child or older parent) develop a respiratory infection. Health class would perhaps better serve their needs if were lighter on the diatribes focused on firearms, water pollution, overeating and refocused on common and predictable issues which drive health care service consumption. For example, perhaps we should impart the know how as to what to measure (temperature, respirations, pulse, BP) and when a visit to an urgent care setting is recommended. What medications should be routinely stocked and used. What to do about dehydration, nausea, vomiting, or diarrhea? Again when and who to call and when an ED visit might be in order.
Redirecting efforts to educate and impart practical knowledge may also establish credibility for health curriculum. Spending time and money trying to focus on convincing people to not do what they want to do is is a recipe for failure. Mixing in some practical knowledge for dealing with issues that make them feel bad is more likely a winner.
Given my own recent experience with parent health issues, I am tempted to also push for inclusion of family health issues into a practical health curriculum. While our own aging will be part of our lives (hopefully), the aging or our parents will almost certainly precede this (barring their or our early demise). Our educational system fails to prepare us in any practical way for either our own or family aging issues. I have my doubts this would be effective. Health curriculum generally includes normal growth and development but oddly enough development seems to stop once adulthood is reached. The absence of any recognition of aging may be justified on the basis that the target audience suffers from the illusion of immortality and this information would fall upon deaf ears. However, the lack of any information acknowledging aging as part of normal development may be part of the problem.
I could go on and on but I won't. There may be exceptions and I would love to be made aware of a curriculum which addresses these more practical considerations. I suspect they are few and far between. There is a common thread which I touched upon in an earlier piece I wrote about medical knowledge vs. know how. We are still experiencing the legacy of the Ancient Greeks and the clash between the philosophies of Sophists focused on practical knowledge and the school of Aristotle and Plato whose focus of education was on the search for timeless and universal truths. Timeless and universal truths are important. For an educational institution they will put you on the map but for the rest of the world, education also needs to transmit practical knowledge. It is the glue that holds complex societies together.
Saturday, December 25, 2010
Friday, December 24, 2010
The value of words - What is Value?
I was in a meeting where we discussed the principles of physician compensation. I am actually very proud of my institution in that it is making a concerted effort to get beyond the focus on financial metrics. However, I again was reminded of the difficulty of getting beyond flaws which reside outside of your individual institution, particularly when they are flaws in how people and organizations are financially rewarded for the work they do. No matter how much we want to rise above financial considerations, we are dependent upon money to fuel the engines that drive health care. While money may not be the sole consideration, when it is in short supply, it becomes the major consideration. And it appears to always be in short supply.
As a surrogate for actual billings and collections, we are moving to the use of RVUs, relative value units. They come across with at least the patina of legitimacy. My problem with RVUs is they have been described as the worst of Boston disguised as the best of Chicago. They use the word value but it begs the question as value to whom? RVUs are calculated based upon the objective theory of value, assuming that the value of any good or service can be determined by measuring the inputs required to produce it. This is a fundamentally flawed assumption. No matter how complex the service delivered to any given patient, if the service does not provide something of value to the patient, it is by definition of no value. It might be argued that RVUs are a useful however rough approximation which may be on average correct. I suspect that a closer approximation to reality is that the value assigned to a given activity is almost never aligned with the value actually garnered by actual recipients.
RVUs may be a useful accounting tools when trying to calculate the value of given activity to a practice or health care organization. However, this is where the term value becomes confusing. When various medical pundits throw out the term "value" in medicine, the implication is they are talking about value to patients. Michael Porter summarizes the challenges well in a recent NEJM piece:
The other term which has ambiguous meaning is the word productivity. Within large integrated healthcare systems, productivity is measured by RVUs billed or collections per FTE. Obviously this is a reasonably good measure of value to the healthcare system in our current environment where providers are "paid per click". This idea of productivity may provide almost no information regarding actual value to patients. I suspect that Dr. Mark Midei was viewed as one of his hospital productivity "stars" right up until the day that he was indicted for Medicare fraud for placing stents in patients who did not need them. Productivity is defined as outpoint (outcomes) per worker per unit of time. From the hospitals perspective, the most readily measured output is the money coming in. More money coming in tracks with greater productivity from their perspective. It is hard to fathom that if money is coming in, there is little or no value being generated. That is why behaviors which appear to be outrageous in retrospect go on for so long. Who is going to pull the emergency stop cable on activities which which the only obvious elements is they are ridiculously lucrative? That they are wasteful and not productive is all a matter of perspective and the most readily measurable elements make them look very productive in real time.
So we are left with ambiguous language and a world where we are waiting for the financial phase shift in health care where we will rapidly go from productivity being viewed as doing as much activity as possible to doing as little as possible and remaining effective. How do you plan for such a transition? As one of my colleagues says, it is like planning to rewire the house with the electricity still live. Maybe it will be easier to simply build a new house or at least create a new wing with a separate fusebox?
As a surrogate for actual billings and collections, we are moving to the use of RVUs, relative value units. They come across with at least the patina of legitimacy. My problem with RVUs is they have been described as the worst of Boston disguised as the best of Chicago. They use the word value but it begs the question as value to whom? RVUs are calculated based upon the objective theory of value, assuming that the value of any good or service can be determined by measuring the inputs required to produce it. This is a fundamentally flawed assumption. No matter how complex the service delivered to any given patient, if the service does not provide something of value to the patient, it is by definition of no value. It might be argued that RVUs are a useful however rough approximation which may be on average correct. I suspect that a closer approximation to reality is that the value assigned to a given activity is almost never aligned with the value actually garnered by actual recipients.
RVUs may be a useful accounting tools when trying to calculate the value of given activity to a practice or health care organization. However, this is where the term value becomes confusing. When various medical pundits throw out the term "value" in medicine, the implication is they are talking about value to patients. Michael Porter summarizes the challenges well in a recent NEJM piece:
The current organizational structure and information systems of health care delivery make it challenging to measure (and deliver) value. Thus, most providers fail to do so. Providers tend to measure only what they directly control in a particular intervention and what is easily measured, rather than what matters for outcomes. For example, current measures cover a single department (too narrow to be relevant to patients) or outcomes for a whole hospital, such as infection rates (too broad to be relevant to patients). Or they measure what is billed, even though current reimbursement practices are misaligned with value. Similarly, costs are measured for departments or billing units rather than for the full care cycle over which value is determined. Faulty organizational structure also helps explain why physicians fail to accept joint responsibility for outcomes, blaming lack of control over “outside” actors involved in care (even those in the same hospital) and patients' compliance.http://www.nejm.org/doi/full/10.1056/NEJMp1011024
The other term which has ambiguous meaning is the word productivity. Within large integrated healthcare systems, productivity is measured by RVUs billed or collections per FTE. Obviously this is a reasonably good measure of value to the healthcare system in our current environment where providers are "paid per click". This idea of productivity may provide almost no information regarding actual value to patients. I suspect that Dr. Mark Midei was viewed as one of his hospital productivity "stars" right up until the day that he was indicted for Medicare fraud for placing stents in patients who did not need them. Productivity is defined as outpoint (outcomes) per worker per unit of time. From the hospitals perspective, the most readily measured output is the money coming in. More money coming in tracks with greater productivity from their perspective. It is hard to fathom that if money is coming in, there is little or no value being generated. That is why behaviors which appear to be outrageous in retrospect go on for so long. Who is going to pull the emergency stop cable on activities which which the only obvious elements is they are ridiculously lucrative? That they are wasteful and not productive is all a matter of perspective and the most readily measurable elements make them look very productive in real time.
So we are left with ambiguous language and a world where we are waiting for the financial phase shift in health care where we will rapidly go from productivity being viewed as doing as much activity as possible to doing as little as possible and remaining effective. How do you plan for such a transition? As one of my colleagues says, it is like planning to rewire the house with the electricity still live. Maybe it will be easier to simply build a new house or at least create a new wing with a separate fusebox?
Thursday, December 23, 2010
Medicare Fraud -The inevitable product of the system designed to deliver fraud
The WSJ just published a piece highlighting unscrupulous billing practices which likely costs Medicare billions of dollars.
http://online.wsj.com/article/SB10001424052748704851204576034332420051722.html.
http://online.wsj.com/article/SB10001424052748704457604576011382824069032.html.
The comments which followed the article fall into the usual finger pointing mode... inept government, unethical providers, FMG's, inevitability due to human nature, etc. I am reminded of the mantra of the healthcare safety movement that unfortunate results are often the result of poor system design which predictably generate undesirable outcomes.
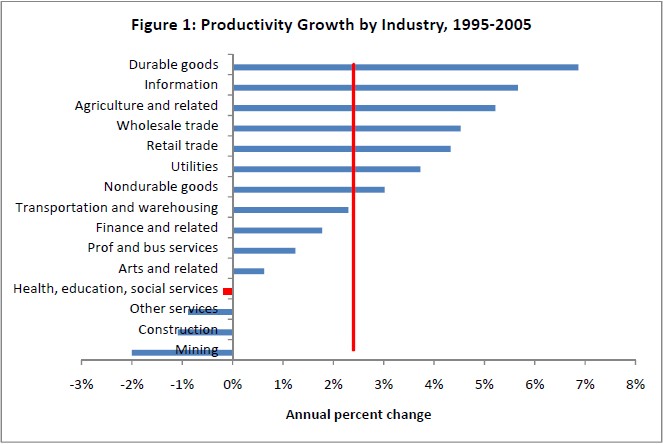
Let us look at the story described in the WSJ article. A particular high profile doc in south Florida aggressively bills Medicare for physical therapy services to the tune of millions of dollars. Our immediate response is this is unscrupulous and he has been gaming the system. This is likely a correct conclusion but perhaps a deeper analysis is warranted. What part of his activities were undesirable? Is it the fact that he was able to project his expertise and services to large numbers of patients? In other realms of business that is viewed rather positively. In fact, one of the major criticisms of the health care industry has been the lack of productivity gains over the past 40 years.
http://theincidentaleconomist.com/wordpress/the-health-care-productivity-problem/

Was he claiming to deliver services when the work was delegated to some other person? That is a possibility but again, where is the harm if the patient actually received and benefited from the service. Is that not gain sharing? Licensing requirements may have been violated but if the patients received the service and benefited from this (and were not harmed), it is more likely that the licensing requirements are serving the provider guilds more than the patients. Delegation to less expensive providers and movement to rules based delivery systems drive productivity gains. If we use volume as a criteria to identify fraud, we will be inadvertently targeting the very entrepreneurial innovators who can lead us to productivity gains.
Was he actually delivering value to the patients that he served? We have absolutely no idea. Here lies the problem. We have deployed a payment system which divorces the payment from the actual delivery of value. This actually is built into the system at multiple levels. First, the actual level of payment for services is set administratively and it is set to a one size fits all. No matter how valuable the service is to any given patient the value to the provider to deliver the service is the same. The pricing system is devoid of differentials to prioritize who should actually receive the service. On one side, this prevents those from who value the service most highly from being priority customers and on the other side, it creates a perverse incentive to deploy the service to even those who will derive little or no value from it.
Even if there was some sort of price differential based upon actual value to the recipient, the insulation of those actually receiving the service from the entities paying for it means there is an almost total loss of discipline in the process. In the case of the physical therapy sessions billed by this Florida physician, which patients are not going to like getting back rubs that they do not pay for. I suspect that if Medicare were to survey the patients who received the services to determine whether they believed they were the victims of fraud, they would likely find very few who believed they had been victims. Even the ones who received no services at all, why should they care? They likely received no bills either. Design a system like this and what do you expect? While at the onset most participants will stay within the lines, it only takes a few "gamers" to discover and exploit the weaknesses. The rest of the world will follow them when they are cautioned not to leave money on the table redefining the bounds of decency as they do so.
The fundamental flaw is the financial triangle. Two way exchanges are not nearly as open to rampant fraud because those who pay are the ones who receive the service. No service, no payment. No payment, no service. The three way is never desirable and even more so in a realm where there are not ready checks and balances. Transaction one is to send the money to some agent whose primary desire is to hold on to the cash. Transaction two is some sort of medical service delivered by an agent who has a motivation to do as many things as possible and convince the recipient of those services that they are necessary and valuable. Transaction three is the claim of the health care provider on some share of the cash accumulated by the payer from transaction one. Distantly linked to the previous transactions are the purchase of health insurance which is temporally divorced from the actual delivery of services and only opaquely linked in terms of cost and use. There are essentially no immediate or delayed rewards for anything resembling good citizenship. Those who come out ahead financially are ones who game early and often. The difference between "legitimate" gaming and fraud is blurring to start with and morphs constantly over time.
The point is there will always be people who game whatever system that exists. Once the pioneers demonstrate that pushing the envelope creates financial windfalls, even those with less entrepreneurial spirit follow their leads. In the marketplace of a price coordinated economy where those who receive the service actually pay for it, fraud exists but it is hard for it to grow to such proportions. People who pay with their own resources are much more prudent in terms of spending. Furthermore, the more people who exploit particular avenues, the greater the availability of particular services and the more the price falls. Systems such as Medicare have few feedback loops to identify real value and have no real time price signals. Supply has little relation to demand. For Medicare, price is simply an accounting device devoid of the ability to coordinate human activity within any meaningful time frame. Providers respond to price by doing more of what drives their margins irrespective of what value is brought to patients.
The talent available looking for points of weakness will always outstrip the ability to detect and respond effectively to fraud. No matter how robust the engineering appears to be, it will always be flawed since it is based upon a foundation which cannot support it.
http://online.wsj.com/article/SB10001424052748704851204576034332420051722.html.
http://online.wsj.com/article/SB10001424052748704457604576011382824069032.html.
The comments which followed the article fall into the usual finger pointing mode... inept government, unethical providers, FMG's, inevitability due to human nature, etc. I am reminded of the mantra of the healthcare safety movement that unfortunate results are often the result of poor system design which predictably generate undesirable outcomes.
Let us look at the story described in the WSJ article. A particular high profile doc in south Florida aggressively bills Medicare for physical therapy services to the tune of millions of dollars. Our immediate response is this is unscrupulous and he has been gaming the system. This is likely a correct conclusion but perhaps a deeper analysis is warranted. What part of his activities were undesirable? Is it the fact that he was able to project his expertise and services to large numbers of patients? In other realms of business that is viewed rather positively. In fact, one of the major criticisms of the health care industry has been the lack of productivity gains over the past 40 years.
http://theincidentaleconomist.com/wordpress/the-health-care-productivity-problem/
Was he claiming to deliver services when the work was delegated to some other person? That is a possibility but again, where is the harm if the patient actually received and benefited from the service. Is that not gain sharing? Licensing requirements may have been violated but if the patients received the service and benefited from this (and were not harmed), it is more likely that the licensing requirements are serving the provider guilds more than the patients. Delegation to less expensive providers and movement to rules based delivery systems drive productivity gains. If we use volume as a criteria to identify fraud, we will be inadvertently targeting the very entrepreneurial innovators who can lead us to productivity gains.
Was he actually delivering value to the patients that he served? We have absolutely no idea. Here lies the problem. We have deployed a payment system which divorces the payment from the actual delivery of value. This actually is built into the system at multiple levels. First, the actual level of payment for services is set administratively and it is set to a one size fits all. No matter how valuable the service is to any given patient the value to the provider to deliver the service is the same. The pricing system is devoid of differentials to prioritize who should actually receive the service. On one side, this prevents those from who value the service most highly from being priority customers and on the other side, it creates a perverse incentive to deploy the service to even those who will derive little or no value from it.
Even if there was some sort of price differential based upon actual value to the recipient, the insulation of those actually receiving the service from the entities paying for it means there is an almost total loss of discipline in the process. In the case of the physical therapy sessions billed by this Florida physician, which patients are not going to like getting back rubs that they do not pay for. I suspect that if Medicare were to survey the patients who received the services to determine whether they believed they were the victims of fraud, they would likely find very few who believed they had been victims. Even the ones who received no services at all, why should they care? They likely received no bills either. Design a system like this and what do you expect? While at the onset most participants will stay within the lines, it only takes a few "gamers" to discover and exploit the weaknesses. The rest of the world will follow them when they are cautioned not to leave money on the table redefining the bounds of decency as they do so.
The fundamental flaw is the financial triangle. Two way exchanges are not nearly as open to rampant fraud because those who pay are the ones who receive the service. No service, no payment. No payment, no service. The three way is never desirable and even more so in a realm where there are not ready checks and balances. Transaction one is to send the money to some agent whose primary desire is to hold on to the cash. Transaction two is some sort of medical service delivered by an agent who has a motivation to do as many things as possible and convince the recipient of those services that they are necessary and valuable. Transaction three is the claim of the health care provider on some share of the cash accumulated by the payer from transaction one. Distantly linked to the previous transactions are the purchase of health insurance which is temporally divorced from the actual delivery of services and only opaquely linked in terms of cost and use. There are essentially no immediate or delayed rewards for anything resembling good citizenship. Those who come out ahead financially are ones who game early and often. The difference between "legitimate" gaming and fraud is blurring to start with and morphs constantly over time.
The point is there will always be people who game whatever system that exists. Once the pioneers demonstrate that pushing the envelope creates financial windfalls, even those with less entrepreneurial spirit follow their leads. In the marketplace of a price coordinated economy where those who receive the service actually pay for it, fraud exists but it is hard for it to grow to such proportions. People who pay with their own resources are much more prudent in terms of spending. Furthermore, the more people who exploit particular avenues, the greater the availability of particular services and the more the price falls. Systems such as Medicare have few feedback loops to identify real value and have no real time price signals. Supply has little relation to demand. For Medicare, price is simply an accounting device devoid of the ability to coordinate human activity within any meaningful time frame. Providers respond to price by doing more of what drives their margins irrespective of what value is brought to patients.
The talent available looking for points of weakness will always outstrip the ability to detect and respond effectively to fraud. No matter how robust the engineering appears to be, it will always be flawed since it is based upon a foundation which cannot support it.
Saturday, December 18, 2010
The pandora's box of sedentism
I recently again listened to the Teaching Company course "Big History" by Professor David Christain. It is an absolutely fascinating series of lectures which take one from the Big Bang to the present day (in 48 lectures). There are so many interesting elements of this course but the one that struck me this time around was the discussion of the concept of sedentism.
Sedentism is defined in Wikipedia as:
The initial transition to sedentism potentially started with cultures who stopped wandering because of they lived in locales where food was so abundant that people could settle down. However, once settled, the trap was sprung. It likely prompted an expansion of population which created imperatives for intensifying exploitation of local resources. Remaining in one place expanded the possibilities for supporting populations which could not survive in a wandering society.
Once a society was constituted to support those who who needed resources they could not generate themselves, it set the stage for a series of moral dilemmas which we are grappling with today. In Natufian culture over 10,000 years ago, the entitlements were likely very modest. Settled people came to accept that they could not leave their elders and family out in the elements and refuse to feed them. While their ancestors were incapable of carrying the old and invalid, the change to a settled people created a whole new world of the possible. Many of the possibilities set the stage for explosive human development. It was at the cost of creating a question which we will grapple with as long as people are around.
The moral imperative to care for those who cannot entirely care for themselves is part of what makes us human. It is not simply a drain on resources but I believe our empathy and willingness to to help sustain others is a key element in the development of complex social and productive networks. However, it consistently places human populations in moral dilemmas where limits must be placed on largess.
Over 10,000 years ago, the transition to sedentism set events in motion which now compel us to scramble for resources to provide complex mix of goods and services (including medical services). Resources will always be scarce in that legitimate wants will always outstrip the resources available to meet them. No longer does it suffice for us to simply provide basic shelter and subsistence diets for those who have limited capacity to generate their own resources. It begs the question (s) - How much or little are people entitled to and why? What is the minimal set of goods and services now? How will this morph over time and how fast? How are these decisions to be made?
These are not easy questions because they have no durable answers. Beware of anyone who who is sure of their answers.
Sedentism is defined in Wikipedia as:
In evolutionary anthropology and archaeology, sedentism (sometimes denominated sedentariness), is a term applied to the transition from nomadic to permanent, year-round settlement.Professor Christain suggests that sedentism was not as simple as nomads settling down when they they figured out how to farm and domesticated animals. He suggests that sedentism was a type of a trap which created a series of moral dilemmas which we are still grappling with today. Nomadic hunter societies simply did not allow anyone the luxury of carrying those who could not carry themselves. It was a cruel world where those who could not travel did not survive.
The initial transition to sedentism potentially started with cultures who stopped wandering because of they lived in locales where food was so abundant that people could settle down. However, once settled, the trap was sprung. It likely prompted an expansion of population which created imperatives for intensifying exploitation of local resources. Remaining in one place expanded the possibilities for supporting populations which could not survive in a wandering society.
Once a society was constituted to support those who who needed resources they could not generate themselves, it set the stage for a series of moral dilemmas which we are grappling with today. In Natufian culture over 10,000 years ago, the entitlements were likely very modest. Settled people came to accept that they could not leave their elders and family out in the elements and refuse to feed them. While their ancestors were incapable of carrying the old and invalid, the change to a settled people created a whole new world of the possible. Many of the possibilities set the stage for explosive human development. It was at the cost of creating a question which we will grapple with as long as people are around.
The moral imperative to care for those who cannot entirely care for themselves is part of what makes us human. It is not simply a drain on resources but I believe our empathy and willingness to to help sustain others is a key element in the development of complex social and productive networks. However, it consistently places human populations in moral dilemmas where limits must be placed on largess.
Over 10,000 years ago, the transition to sedentism set events in motion which now compel us to scramble for resources to provide complex mix of goods and services (including medical services). Resources will always be scarce in that legitimate wants will always outstrip the resources available to meet them. No longer does it suffice for us to simply provide basic shelter and subsistence diets for those who have limited capacity to generate their own resources. It begs the question (s) - How much or little are people entitled to and why? What is the minimal set of goods and services now? How will this morph over time and how fast? How are these decisions to be made?
These are not easy questions because they have no durable answers. Beware of anyone who who is sure of their answers.
Subscribe to:
Comments (Atom)