
I mopped up my aging messages in my message box yesterday with the hope that I could take care of everything that was pressing before the holidays. I called one particular patient whose message intimated that he had suffered a complication from a recent treatment. This was a patient who I have followed for years from a variety of chronic conditions. I had seen him in the office more than a dozen times.
My impression of him from these generally brief encounters was that he was a pleasant man, rarely appearing in any distress. I knew he traveled from a modest distance and most recently, we had elected to have his care transferred to a facility closer to his home. He was approaching his 9th decade of life and suffering from a number of slowly debilitating conditions which made travel increasingly difficult, particularly a chronic neuro-degenerative disease. Still, from all outward signs, he appeared to be quite intact and robust.
I called him at home to inquire as to the nature of extent of his difficulties. As it turned out, he was feeling fine and the issues that initially prompted his call were sell on the way to resolution. However, the opportunity to speak to me in the relatively unhurried context of my call created an opportunity for him to share a whole host of questions and long standing issues. I listened intently.
As it turned out that despite seeing this gentleman repeatedly over many years, I hardly knew him at all. He was retired from the aerospace industry, something I had no inkling of. He was a keen observer of detail, recalling specific details of past encounters, particularly actions we did which were inconsistent over time. He noted variation in our staff activities, instructions they gave, and issues that appeared to develop as a consequence. He was a wealth of information which we might have benefited from if we had only listened to him.
As the conversation went on, he also went on to share some of the challenges he faced now with an ailing spouse and growing costs of her care. The time and financial burdens were actually rather staggering. I hadn't a clue as to what he faced. I began to wonder whether the incremental benefits he might derive from our frequent interventions might be viewed as not worth his investment of time and money compared to the benefits he might have received from investing his time and money elsewhere. Those considerations were never on my radar. I had what amounted to be an incomplete context to place my recommendations into.
As individual physicians what are our obligations to know these types of details regarding our patients? In the current model, it is simply not practical to delve into this type of detail and there are no incentives to do so. In reality, there are huge financial incentives to remain as ignorant as possible. Injection of personal complexities into the production model of medicine slows decision making, taking decisions which might be viewed in black and white terms to shades of gray. Shades of gray may not be compatible with efficiency, a euphemism for speed and throughput.
Can we actually do our jobs well if no one in the medical community deals with this? Is this a personal responsibility of patients to make their preferences known or at least delegate a family member or friend to advocate? I can't say for certain who should do this but it is reasonable to assume there are multiple possible approaches, most of which will not be deployed in our current system because they cannot be readily monetized. We can hope that such time consuming and complex activities will be available broadly based upon the spirit of volunteerism, but this represents a best can be described as an aspiration for the triumph of hope over experience.
Improvement in the delivery of health care ultimately requires better decision making and those decisions require a better understanding of the unique goals of individuals. If we representing those who assist in making those decisions are near complete strangers to those they are assisting, we will not be in a position to provide optimal guidance and perhaps will provide more bad advice than good.
Saturday, December 22, 2012
Saturday, December 15, 2012
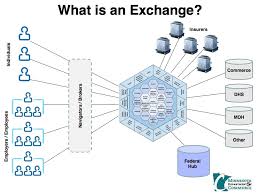
The fallacies of intelligent Design - Unintended consequences and health insurance exchanges
In a previous blog, I noted that a fundamental difference between conservatives and liberals is that the later tend to focus on what should be while the former tend to focus on what can be. Perhaps no where is this now more evident than in the developing story on the deployment of health insurance exchanges. The ACA timetable for deployment of the exchanges calls for them to deployed and operational by October of 2013. it is now appearing increasingly unlikely that this has any real hope of actually happening. 
The NYT reported yesterday that it is likely that only 17 states will operate their own exchanges. As noted in the article by Robert Fear:
The remainder have chosen to forego this opportunity. The reasons are multiple but a common theme appears to be the lack of guidance which was forthcoming from the Washington DC bureaucracy. As noted the the NYT piece:
I have no particular desire to gloat. Innumerable patients I care for have taken this timetable to heart and are betting on the timely access to insurance which will provide them with affordable coverage independent of pre-existing conditions. I am concerned they have placed their hopes on something many would consider desirable but is not not feasible. Both are required.
When Nancy Pelosi proclaimed that the bill needed to be passed in order to see what what in it, it turns out she was not kidding. At the time the thought was that she was referring to the extensive document already written. However, this aspirational document represented only a shell of what will ultimately be needed. What appeared to be a good and grand idea gets a bit more complicated when the idea is to reconstitute perhaps 20% of the economy and make it micromanaged by federal bureaucrats.
This episode adds new meaning to the term "Intelligent Design". When political officials express skepticism regarding biological evolution and embrace concepts that the universe can and was designed by some intelligent being, they are ridiculed a being ignorant. I agree that those views are ridiculous and should be challenged. Complexity and durable complex systems do not develop as a consequence of top down architects.
Similarly, when human beings try to assume they can take on god like powers they are behaving in an ignorant fashion. I am sure that when HHS took on the task of simply providing guidance to states trying to build exchanges, they quickly found themselves in over their heads. No gods or intelligent design capacity there. I hate to imagine what they have ahead of them when they attempt to build exchanges for the remaining 33 states. These are entities which can evolve over time if the appropriate rules and selection pressures are applied. I have my doubts they can be the product of creation by people and institutions which are made of ordinary people.
The NYT reported yesterday that it is likely that only 17 states will operate their own exchanges. As noted in the article by Robert Fear:
The federal government and states face a series of deadlines in the new year. On Jan. 1, Secretary Sebelius must determine whether each state will be able to operate its own exchange in compliance with federal standards. By Feb. 15, states must notify the federal government if they want to help with selected tasks, like consumer assistance and the supervision of health plans, in partnership with the federal government.
On Oct. 1, consumers can begin to enroll in health plans, for coverage starting on Jan. 1, 2014, when most Americans will be required to have insurance.
The remainder have chosen to forego this opportunity. The reasons are multiple but a common theme appears to be the lack of guidance which was forthcoming from the Washington DC bureaucracy. As noted the the NYT piece:
In Tennessee, state officials did a huge amount of planning for a state-run exchange. But Gov. Bill Haslam announced this week that he had decided against the idea because the Obama administration had failed to answer numerous operational questions.
Gov. Chris Christie of New Jersey cited similar concerns in vetoing legislation to establish a state-based exchange last week.
“New guidance continues to trickle out of Washington at an erratic pace,” Mr. Christie said.
I have no particular desire to gloat. Innumerable patients I care for have taken this timetable to heart and are betting on the timely access to insurance which will provide them with affordable coverage independent of pre-existing conditions. I am concerned they have placed their hopes on something many would consider desirable but is not not feasible. Both are required.
When Nancy Pelosi proclaimed that the bill needed to be passed in order to see what what in it, it turns out she was not kidding. At the time the thought was that she was referring to the extensive document already written. However, this aspirational document represented only a shell of what will ultimately be needed. What appeared to be a good and grand idea gets a bit more complicated when the idea is to reconstitute perhaps 20% of the economy and make it micromanaged by federal bureaucrats.
This episode adds new meaning to the term "Intelligent Design". When political officials express skepticism regarding biological evolution and embrace concepts that the universe can and was designed by some intelligent being, they are ridiculed a being ignorant. I agree that those views are ridiculous and should be challenged. Complexity and durable complex systems do not develop as a consequence of top down architects.
Similarly, when human beings try to assume they can take on god like powers they are behaving in an ignorant fashion. I am sure that when HHS took on the task of simply providing guidance to states trying to build exchanges, they quickly found themselves in over their heads. No gods or intelligent design capacity there. I hate to imagine what they have ahead of them when they attempt to build exchanges for the remaining 33 states. These are entities which can evolve over time if the appropriate rules and selection pressures are applied. I have my doubts they can be the product of creation by people and institutions which are made of ordinary people.
The Pain of the Hedgehog
In today's Wall Street Journal, there was a very interesting article focusing on Dr. Russel Portenoy. (Portenoy) Dr. Portenoy was a instrumental driver of a movement in medicine to address the under treatment of pain. I remember this movement at or near its inception and have to admit it made sense to me at the time and for the most part, it still resonates, although mostly as it relates to acute pain.

Early in his career Dr. Portenoy had a big idea. He noted that opiates were extremely effective in the management of pain in patients affected with cancer. He envisioned that these drugs could be used in a much broader clinical context to treat chronic pain in patients who did not have cancer. He was very smart, and very articulate and these elements mixed with his passion for for what her believed in catapulted his agenda to the front and center of medicine and the public. He changed how medicine was practiced.
He was a hedgehog. Isaiah Berlin in his essay the "Hedgehog and the Fox" borrowed from the Greek Archilocus, to divide thinkers into two categories, hedgehogs and foxes. Hedgehogs believe single defining ideas while foxes draw on a much larger set of experiences and hold more skepticism that we can place as much stock in any single idea. Hedgehogs are much better positioned to move the needle on any given issue. They are better advocates because they tend not to be distracted by anything, including evidence which fails to support their big idea.
Dr. Pourtnoy overcame resistance to wider use of opiates using his powers of persuasion to convince skeptics that the dangers of opiate use were overstated. He believed at the time that the evidence did not support the concerns which had long limited their use. While he may have correct that the evidence did not support the dangers, his hedgehog biases also blinded him to the lack of evidence supporting their safe long term use. He confused strong belief with strong evidence. To his credit, he now appears to have recognized that his efforts have resulted in substantial unintended consequences and he would not have pursued the same agenda if he knew at the movement's inception what he now know now.
The world needs both hedgehogs and foxes. Too many foxes and no one will pursue big and bold ideas. However, too many hedgehogs results in too many big gambles. Furthermore, it also makes a difference where the hedgehogs and foxes reside.
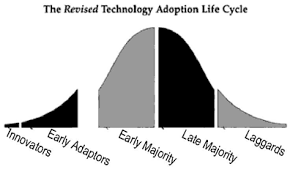
Within our world, we have people who are early adopters and others who are late adopters. That mix is great for creating "unfragile" entities. Early adopter can hit it big or can go down in flames. Late adopters can be so conservative that they relegate themselves to oblivion or they can serve as a reservoir to repopulate after the early adopters have done something crazy. It works because you have diverse groups hedging their bets in lots of different ways.
However, put a hedgehog in a position of authority and in charge of some entity which can compel others to uniformly embrace big ideas and you remove that diversity of response. In the world of pain management, the hedgehogs captured the power of medical licensing boards and used coercive tools to push their big idea.
 I have to admit I have my hedgehog tendencies, particularly relating to the deployment of data and data tools in medicine. It is my big idea (although do not take that to mean I conceived this). I think big ideas are fine as long as they are pursued within a particular framework. First, if at all possible, big ideas need to be pushed out within an environment where people have the right to decline them. No matter how good the idea sounds, it is desirable to have cadres of people who are free to reject them and exercise that freedom, even if they appear to be stupid at the time. Second, big ideas should be deployed in an environment which has feedback loops already in place. The concepts of improvement and progress are meaningless if there are no mechanisms in place to define where you started from and where you ended up. Finally, understanding success or failure, improvement, and unintended consequences often requires a time frame which is beyond the attention span of individuals or individual human lifetimes. What appears to be success after a few months or years, can translate into disaster after a few decades.
I have to admit I have my hedgehog tendencies, particularly relating to the deployment of data and data tools in medicine. It is my big idea (although do not take that to mean I conceived this). I think big ideas are fine as long as they are pursued within a particular framework. First, if at all possible, big ideas need to be pushed out within an environment where people have the right to decline them. No matter how good the idea sounds, it is desirable to have cadres of people who are free to reject them and exercise that freedom, even if they appear to be stupid at the time. Second, big ideas should be deployed in an environment which has feedback loops already in place. The concepts of improvement and progress are meaningless if there are no mechanisms in place to define where you started from and where you ended up. Finally, understanding success or failure, improvement, and unintended consequences often requires a time frame which is beyond the attention span of individuals or individual human lifetimes. What appears to be success after a few months or years, can translate into disaster after a few decades.
Early in his career Dr. Portenoy had a big idea. He noted that opiates were extremely effective in the management of pain in patients affected with cancer. He envisioned that these drugs could be used in a much broader clinical context to treat chronic pain in patients who did not have cancer. He was very smart, and very articulate and these elements mixed with his passion for for what her believed in catapulted his agenda to the front and center of medicine and the public. He changed how medicine was practiced.
He was a hedgehog. Isaiah Berlin in his essay the "Hedgehog and the Fox" borrowed from the Greek Archilocus, to divide thinkers into two categories, hedgehogs and foxes. Hedgehogs believe single defining ideas while foxes draw on a much larger set of experiences and hold more skepticism that we can place as much stock in any single idea. Hedgehogs are much better positioned to move the needle on any given issue. They are better advocates because they tend not to be distracted by anything, including evidence which fails to support their big idea.
Dr. Pourtnoy overcame resistance to wider use of opiates using his powers of persuasion to convince skeptics that the dangers of opiate use were overstated. He believed at the time that the evidence did not support the concerns which had long limited their use. While he may have correct that the evidence did not support the dangers, his hedgehog biases also blinded him to the lack of evidence supporting their safe long term use. He confused strong belief with strong evidence. To his credit, he now appears to have recognized that his efforts have resulted in substantial unintended consequences and he would not have pursued the same agenda if he knew at the movement's inception what he now know now.
The world needs both hedgehogs and foxes. Too many foxes and no one will pursue big and bold ideas. However, too many hedgehogs results in too many big gambles. Furthermore, it also makes a difference where the hedgehogs and foxes reside.
Within our world, we have people who are early adopters and others who are late adopters. That mix is great for creating "unfragile" entities. Early adopter can hit it big or can go down in flames. Late adopters can be so conservative that they relegate themselves to oblivion or they can serve as a reservoir to repopulate after the early adopters have done something crazy. It works because you have diverse groups hedging their bets in lots of different ways.
However, put a hedgehog in a position of authority and in charge of some entity which can compel others to uniformly embrace big ideas and you remove that diversity of response. In the world of pain management, the hedgehogs captured the power of medical licensing boards and used coercive tools to push their big idea.
Sunday, November 18, 2012
Diagnostic Error
I attended the meeting of the Society for Improved Diagnosis in Medicine this past week in Baltimore. This is a new society, being formally constituted within the past year, although this was the fifth meeting. Previously it had met with other groups, most recently the Society of Medical Decision making.

The major focus was one developing tools and approaches to define the scope of the problem which likely huge but difficult to define and quantify. It was a fascinating group of people which included physicians from a host of specialties. However, it was not limited to physicians and I would venture to guess that nearly half (and perhaps more than half) of the attendees were non-physicians, including many patients.
Even that characterization is not entirely accurate since every one of the attendees are currently recipients of some form of medical care, some more intensively than others. This is of note in that all inquiries into the sources diagnostic error and approaches to addressing diagnostic error interested with the patient communities. Their stories of harm were compelling and at times overwhelming. Their stories were not an add-on to the meeting but in fact central to it.
I was struck by the gulf that still separates patients from physicians and the health care delivery system, a gulf that is maintained by perceptions, processes, and desires to maintain power. However, as I heard the stories of patients, many of whom were very smart and sophisticated, I realized that the elements which maintain the separateness are the same elements which are a source of diagnostic error in the first place.
My perspective as a physician is shaped by the perceptions of those I trained with and those I work with. We view patient histories with great skepticism. What we hear from patients may not be accurate, relevant, or complete. That may be because they do not give us complete stories, not surprising since we demand they provide them under the most time constrained conditions where they suffer from significant performance anxiety. It may also because we fail to hear what they are trying to say and fail to give them sufficient time to reflect upon what the feedback we give them.

My residents often complain that I am able to elicit a history different from what they obtain. I found this very curious until I had a realization as to why this happens. Resident interviews act as a facilitator for patients to reflect upon what we as physicians want to know. Patients come into visits as poorly prepared as we do an questions offered by the residents surprise them. Answers obtained under those circumstances are often incomplete or wrong. However, in the time supplied after the resident leaves and I arrive, patients reflect and rethink their answers, having time to get their stories straight. No guile involved; just the opportunity for reflection improves the quality of the information delivered.
There were lots of interesting aspects of the conference and many interesting speakers. However, one specific session made a particular impression. It was very focused on the role of patients in addressing diagnostic error. The roles proposed proposed for patients raised in my mind the thought that addressing the problem of diagnostic error will require a fundamental change in how we view the role of patients in the diagnostic process. In each of the patient stories of missed diagnosis the opportunities for improvement and avoidance of similar events appeared to require an engaged and activated patient providing a feedback loop to the health care provider to avoid diagnostic pitfalls.
Once the patient is viewed as part of the diagnostic team, it creates the need to define boundaries and ownership. It was absolutely fascinating to hear the divergence of opinions between the physician and patient communities on where these boundaries should be and there was great concern that the unintended consequences of unfiltered information sharing could be dire. However, it was also pointed out that we survived having family access to delivery rooms and ICUs and that patient and family involvement has turned out to be an enhancement, not a detriment to healthcare delivery.

There is no question in my mind that the old model of care delivery has a short half-life. Patients want and deserve better .However, one particular attendee who was a primary care MD spoke up. He was a bit annoyed the primary care physicians were often pilloried as central characters in stories of harm. He urged patients to ask why their primary care physicians cut them short, ignored their complaints, and appeared to be unsympathetic. Providing thoughtful and reflective care using shared decision making takes time and effort. That fall squarely in the uncompensated or poorly compensated quadrant of physician efforts.
Most of the stories of harm and missed diagnosis could be linked back to insufficient time to hear or assimilate information from patients and to integrate all of the pieces. Circumstances and models where this does not happen now generally involve heroic efforts of extraordinary people and non-scalable or sustainable models of care. Patients may want and deserve better, but patient leaders need to understand they are dealing with an economic problem. The current administrative pricing structure in health care values physician activities required for reflective and shared care at essentially nothing. The price signals linked to these activities are telling doctors that there is no value in these activities and against this relentless tide of pressure, no one but the most heroic of physicians continues to resist.

Economic laws are almost as immutable as the law of gravity. It takes much energy to keep things from falling. Items valued as nothing tend to disappear over time. It is not surprising we have found ourselves with a scarcity of reflection and time spent with those who patients believe should be their advocates and counselors. Our own moral compasses as physicians tell us when we have time to reflect that we should provide this time to patients, whether we are paid to do so or not. However, that is simply unrealistic. As things stand now, we are the engines that support not only ourselves but entire teams of people who are almost completely dependent upon the revenue generating capacity of physicians. Thus, we make compromises and rationalize these decisions on the basis that overall we do overwhelmingly more good than harm and it is important to keep the lights on and the doors open. We do our own little bits of God's work and recognize that we cannot fix all of the world's ills.

The payment system that fails to incentivize physicians to deliver what is needed to address diagnostic error continues and, for the most part, few recognize that the scarcity has been created by the dysfunctional administrative pricing system. While patient engagement is an essential piece to address diagnostic error, it is necessary but not sufficient. Patient engagement creates activated patients. However, this is of limited utility without activated clinicians. Some clinicians will become activated because of their moral compass but for the broader provider audience, activation will require financial rewards or at least the lack of financial deterrents. The sooner the activated patients realize this, the better off they will be.
The major focus was one developing tools and approaches to define the scope of the problem which likely huge but difficult to define and quantify. It was a fascinating group of people which included physicians from a host of specialties. However, it was not limited to physicians and I would venture to guess that nearly half (and perhaps more than half) of the attendees were non-physicians, including many patients.
Even that characterization is not entirely accurate since every one of the attendees are currently recipients of some form of medical care, some more intensively than others. This is of note in that all inquiries into the sources diagnostic error and approaches to addressing diagnostic error interested with the patient communities. Their stories of harm were compelling and at times overwhelming. Their stories were not an add-on to the meeting but in fact central to it.
I was struck by the gulf that still separates patients from physicians and the health care delivery system, a gulf that is maintained by perceptions, processes, and desires to maintain power. However, as I heard the stories of patients, many of whom were very smart and sophisticated, I realized that the elements which maintain the separateness are the same elements which are a source of diagnostic error in the first place.
My perspective as a physician is shaped by the perceptions of those I trained with and those I work with. We view patient histories with great skepticism. What we hear from patients may not be accurate, relevant, or complete. That may be because they do not give us complete stories, not surprising since we demand they provide them under the most time constrained conditions where they suffer from significant performance anxiety. It may also because we fail to hear what they are trying to say and fail to give them sufficient time to reflect upon what the feedback we give them.
My residents often complain that I am able to elicit a history different from what they obtain. I found this very curious until I had a realization as to why this happens. Resident interviews act as a facilitator for patients to reflect upon what we as physicians want to know. Patients come into visits as poorly prepared as we do an questions offered by the residents surprise them. Answers obtained under those circumstances are often incomplete or wrong. However, in the time supplied after the resident leaves and I arrive, patients reflect and rethink their answers, having time to get their stories straight. No guile involved; just the opportunity for reflection improves the quality of the information delivered.
There were lots of interesting aspects of the conference and many interesting speakers. However, one specific session made a particular impression. It was very focused on the role of patients in addressing diagnostic error. The roles proposed proposed for patients raised in my mind the thought that addressing the problem of diagnostic error will require a fundamental change in how we view the role of patients in the diagnostic process. In each of the patient stories of missed diagnosis the opportunities for improvement and avoidance of similar events appeared to require an engaged and activated patient providing a feedback loop to the health care provider to avoid diagnostic pitfalls.
Once the patient is viewed as part of the diagnostic team, it creates the need to define boundaries and ownership. It was absolutely fascinating to hear the divergence of opinions between the physician and patient communities on where these boundaries should be and there was great concern that the unintended consequences of unfiltered information sharing could be dire. However, it was also pointed out that we survived having family access to delivery rooms and ICUs and that patient and family involvement has turned out to be an enhancement, not a detriment to healthcare delivery.

There is no question in my mind that the old model of care delivery has a short half-life. Patients want and deserve better .However, one particular attendee who was a primary care MD spoke up. He was a bit annoyed the primary care physicians were often pilloried as central characters in stories of harm. He urged patients to ask why their primary care physicians cut them short, ignored their complaints, and appeared to be unsympathetic. Providing thoughtful and reflective care using shared decision making takes time and effort. That fall squarely in the uncompensated or poorly compensated quadrant of physician efforts.
Most of the stories of harm and missed diagnosis could be linked back to insufficient time to hear or assimilate information from patients and to integrate all of the pieces. Circumstances and models where this does not happen now generally involve heroic efforts of extraordinary people and non-scalable or sustainable models of care. Patients may want and deserve better, but patient leaders need to understand they are dealing with an economic problem. The current administrative pricing structure in health care values physician activities required for reflective and shared care at essentially nothing. The price signals linked to these activities are telling doctors that there is no value in these activities and against this relentless tide of pressure, no one but the most heroic of physicians continues to resist.
Economic laws are almost as immutable as the law of gravity. It takes much energy to keep things from falling. Items valued as nothing tend to disappear over time. It is not surprising we have found ourselves with a scarcity of reflection and time spent with those who patients believe should be their advocates and counselors. Our own moral compasses as physicians tell us when we have time to reflect that we should provide this time to patients, whether we are paid to do so or not. However, that is simply unrealistic. As things stand now, we are the engines that support not only ourselves but entire teams of people who are almost completely dependent upon the revenue generating capacity of physicians. Thus, we make compromises and rationalize these decisions on the basis that overall we do overwhelmingly more good than harm and it is important to keep the lights on and the doors open. We do our own little bits of God's work and recognize that we cannot fix all of the world's ills.
The payment system that fails to incentivize physicians to deliver what is needed to address diagnostic error continues and, for the most part, few recognize that the scarcity has been created by the dysfunctional administrative pricing system. While patient engagement is an essential piece to address diagnostic error, it is necessary but not sufficient. Patient engagement creates activated patients. However, this is of limited utility without activated clinicians. Some clinicians will become activated because of their moral compass but for the broader provider audience, activation will require financial rewards or at least the lack of financial deterrents. The sooner the activated patients realize this, the better off they will be.
Saturday, November 17, 2012
Turning the EHR into a project management tool
I have spent a few hours this morning finishing my notes from my clinic yesterday. It occurred to me that for each patient when my note was completed, I had a series of tasks which needed to be done in the future. However, the EHR I use is really poorly equipped to aid me in tracking my future tasks.
EHR's still tend to be used as documentation tools as opposed to something that adds value by helping our brains remember what needs to be done, what has been done, and helping us decide what should be done. There are circumstances where the EHR needs to function simply as a note generator, but that really barely touches upon where it can provide value.
For each patient who I follow long term, I need the equivalent of a project management tool since in many respect, the care of each patient is a long term project. For each patient I need to define what is on my to do list, what am I in the midst of doing, what specific action items are on my plate, and what have I delegated to someone else. At this point in time, the EHR I use does none of this well and many of the tasks it simply has no functionality to use.
Hard to believe that we continue to use such dysfunctional management tools.
EHR's still tend to be used as documentation tools as opposed to something that adds value by helping our brains remember what needs to be done, what has been done, and helping us decide what should be done. There are circumstances where the EHR needs to function simply as a note generator, but that really barely touches upon where it can provide value.
For each patient who I follow long term, I need the equivalent of a project management tool since in many respect, the care of each patient is a long term project. For each patient I need to define what is on my to do list, what am I in the midst of doing, what specific action items are on my plate, and what have I delegated to someone else. At this point in time, the EHR I use does none of this well and many of the tasks it simply has no functionality to use.
Hard to believe that we continue to use such dysfunctional management tools.
Wednesday, November 14, 2012
Medical Reformation
500 years ago, Martin Luther nailed his 95 thesis on the door of the local cathedral.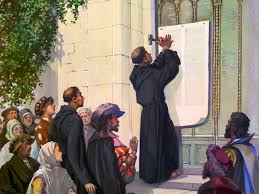
What this event marked was a dramatic change in the relationship of people with the most important human institution in western Europe at the time; the catholic church. Luther's actions was preceded by key technological advances of the day, most notably the development of the printing press by Gutenburg. Prior to the printing press, the church through the clergy controlled access to the printed word, primarily in the form of the bible. After deployment of the printing press, the holy bible, and all of the wisdom contained, was no longer was controlled by the priesthood. Then as now, he who controlled information controlled power.
Prior to the printing press, the church through the clergy controlled access to the printed word, primarily in the form of the bible. After deployment of the printing press, the holy bible, and all of the wisdom contained, was no longer was controlled by the priesthood. Then as now, he who controlled information controlled power.
Roll the clock forward to the last century. The status of physicians in the 20th century underwent a profound change. In the previous century, physicians held a status only slightly higher than barbers. With notable exceptions, most physicians has limited useful knowledge and few tools to deploy when confronted with serious medical situations. The developments of anesthesia, antisepsis, and antibiotics changed all that and by the mid portion of the 20th century, physicians held the status of gods. As Arthur C. Clark once noted, “When technology becomes sufficiently advanced, it becomes indistinguishable from magic”, and medical magic for most of the 20th century held the public is complete awe.
The continuation of awe was also facilitated by the relatively proprietary nature of the knowledge base behind which the medical magicians practiced. We held our cards close and as a rule the public was sufficiently intimidated to inquire further or question physician status.
The internet has begun to change all of this.
Like the printing press, it has taken cloistered texts and other writings out of the hands of the clergy, in this case the medical clergy, and made it available to all those who can search and read. The impact is profound and likely to become even more profound. Prior to the reformation, the catholic church firmly held to the belief that the bible and the information it contained was best controlled by the Church. So much was at stake, that being the souls and eternal fates of human beings. People simply could not be trusted with such responsibilities. Only the special priest class could be entrusted with such a role.
The arguments are being put forth by the medical priesthood. Too much as stake, and patients cannot be entrusted with their own lives. However, the genie is out of the bottle. The information is already out there and more will become available to patients every day. Some of it may be unreliable but the same can be said for what is vetted by peer review in our own fields. Furthermore, patients have an inherent advantage over their health care providers. They have much more time to invest in their own care and they have so much more skin in the game.
I saw the Medical Luthers posting their 95 theses on the door today. They are doing it everywhere. There may be health care providers who will excommunicate their Luthers. I am not sure they have much leverage. The relationship is going to be changed forever.
What this event marked was a dramatic change in the relationship of people with the most important human institution in western Europe at the time; the catholic church. Luther's actions was preceded by key technological advances of the day, most notably the development of the printing press by Gutenburg.
Roll the clock forward to the last century. The status of physicians in the 20th century underwent a profound change. In the previous century, physicians held a status only slightly higher than barbers. With notable exceptions, most physicians has limited useful knowledge and few tools to deploy when confronted with serious medical situations. The developments of anesthesia, antisepsis, and antibiotics changed all that and by the mid portion of the 20th century, physicians held the status of gods. As Arthur C. Clark once noted, “When technology becomes sufficiently advanced, it becomes indistinguishable from magic”, and medical magic for most of the 20th century held the public is complete awe.
The continuation of awe was also facilitated by the relatively proprietary nature of the knowledge base behind which the medical magicians practiced. We held our cards close and as a rule the public was sufficiently intimidated to inquire further or question physician status.
The internet has begun to change all of this.
Like the printing press, it has taken cloistered texts and other writings out of the hands of the clergy, in this case the medical clergy, and made it available to all those who can search and read. The impact is profound and likely to become even more profound. Prior to the reformation, the catholic church firmly held to the belief that the bible and the information it contained was best controlled by the Church. So much was at stake, that being the souls and eternal fates of human beings. People simply could not be trusted with such responsibilities. Only the special priest class could be entrusted with such a role.
The arguments are being put forth by the medical priesthood. Too much as stake, and patients cannot be entrusted with their own lives. However, the genie is out of the bottle. The information is already out there and more will become available to patients every day. Some of it may be unreliable but the same can be said for what is vetted by peer review in our own fields. Furthermore, patients have an inherent advantage over their health care providers. They have much more time to invest in their own care and they have so much more skin in the game.
I saw the Medical Luthers posting their 95 theses on the door today. They are doing it everywhere. There may be health care providers who will excommunicate their Luthers. I am not sure they have much leverage. The relationship is going to be changed forever.
Sunday, November 11, 2012
Speaking different languages about health care as a right
Now that the 2012 elections are over, there is a tendency for those whose perspective is more statist to view that they have received a mandate to go forward with their vision of health care reform. From my perspective, the election provides only the starkest of evidence of a closely divided country where a slim majority supported President Obama's vision of state driven health care changes.
Do not get me wrong. Our present system is terribly flawed and the trajectory of spending is unsustainable. There are constituencies who are committed to holding patterns attempting to extract as many rents from the current system as possible, hoping they can reach retirement age before their goose that lays golden eggs goes away. However, among virtually all thoughtful people there is almost complete agreement that what we are doing presently is not viable in the longer term. The issue is not whether change will happen but instead what that change will look like and who or what will drive it.
President Obama and his supporters tend to hold a belief system which places great confidence in the ability of the law to drive change and to structure human systems in such a way to that law is always a positive force. This belief system is predicated on the assumption that what is most important is the intent of the law and that smart people are fully capable of creating rules, often very complex, which can predictably result in improved incentives and improved outcomes. I should also note that professional politicians on both sides of the isle share this set of assumptions, albeit they may have different levels of confidence that the law can be used in different realms to coerce people to behave. Elements of both the left and the right can be all to willing to seize the reigns of a coercive state into order to bully other elements of the populace.
As I see this, the fundamental gulf that exists revolves around what groups view as the priorities of what the governing leadership should be. What are currently viewed as liberals or progressives (and I hate these terms) prioritize moving toward a world which should exists while conservatives (which is what I view myself as being) place priorities on moving toward a similar world but constrained by what can be. As I wrote about in an earlier blog, von Mises noted in his work "Human Action" (https://www.blogger.com/blogger.g?blogID=2308282620289958037#editor/target=post;postID=7269024980841579619), there is really little disagreement on the articulated goals of:
To me, the most important discussions should focus not on what we aim to achieve but instead on what is actually possible. Going all in aspiring to use the power of the state in order to strive toward a perfect world may sound good, but this experiment has been tried before. The product was not perfection but was instead perfectly awful. What limits our actions in regards to delivery of health care and specifically, what are the limits on state action? Why can't the state use the power of law to simply declare that health care is a right and that ALL those within the borders of the US should have access to health care?
Obviously entire books have been devoted to this and I will not exhaustively delve into all aspects of this question in this essay. The undisputed fact that so much has been and continues to be written belies the complexity involved. However, at the simplest level, you cannot mandate access to what you cannot define, particularly when the definition of what you are referring to is constantly morphing and evolving. Making something a legal right backed by the coercive power of the state requires that you must define the scope of that right. Decentralized private markets and charities are much more nimble in this regard. What one party does at any given time can be distinctly different from other parties involved in similar activities. This is not the case for legal rights. If one cannot define the nature of the right involved, it moves the action, however desirable at a theoretical basis, into the realm of practically impossible. Every decision regarding what is covered can be moved from the personal and medical into the legal realm. If you don't believe this will become unmanageable almost immediately, please refer to the case of Michelle Koselek in Massacheusettes (http://www.cbsnews.com/8301-201_162-57520960/mass-officials-to-fight-murderers-sex-change/).
The issues with defining the scope of any health care right was recently highlighted in the NEJM (http://www.nejm.org/doi/full/10.1056/NEJMp1208386)in a piece by Neuman and Chambers entitled "Medicare's Enduring Struggle to define Reasonable and Necessary Care". In the article the authors note:
Neither necessary of reasonable is definable in any way meaningful way which will create any enduring structure which can address allocation of scarce resources. Neuman and Chambers dance around this issue and conclude by noting:
Thus they admit that the creation of Medicare requires implementation of one size fits all approaches to defining scope. Where will those decisions be made? Whatever the initial intentions of those charged with defining and implementation will be co opted in the realm where all government decisions are made; the political realm. Political allocation of resources yields decisions which generate votes. The political realm works in a winner take all environment where those who can muster tiny majorities can impose their wills on substantial minorities, even if their governance may be unwise.
If the purpose of actions is to strive toward some ideal, whether effective or not, then aspiration alone can be a measure of success. However, I aim for more and am fearful of Utopian aspirations used to justify concentrations of power as a means to attempt what may be theoretically desirable but is almost certainly not attainable in the world of imperfect humans playing politics.
Do not get me wrong. Our present system is terribly flawed and the trajectory of spending is unsustainable. There are constituencies who are committed to holding patterns attempting to extract as many rents from the current system as possible, hoping they can reach retirement age before their goose that lays golden eggs goes away. However, among virtually all thoughtful people there is almost complete agreement that what we are doing presently is not viable in the longer term. The issue is not whether change will happen but instead what that change will look like and who or what will drive it.
President Obama and his supporters tend to hold a belief system which places great confidence in the ability of the law to drive change and to structure human systems in such a way to that law is always a positive force. This belief system is predicated on the assumption that what is most important is the intent of the law and that smart people are fully capable of creating rules, often very complex, which can predictably result in improved incentives and improved outcomes. I should also note that professional politicians on both sides of the isle share this set of assumptions, albeit they may have different levels of confidence that the law can be used in different realms to coerce people to behave. Elements of both the left and the right can be all to willing to seize the reigns of a coercive state into order to bully other elements of the populace.
As I see this, the fundamental gulf that exists revolves around what groups view as the priorities of what the governing leadership should be. What are currently viewed as liberals or progressives (and I hate these terms) prioritize moving toward a world which should exists while conservatives (which is what I view myself as being) place priorities on moving toward a similar world but constrained by what can be. As I wrote about in an earlier blog, von Mises noted in his work "Human Action" (https://www.blogger.com/blogger.g?blogID=2308282620289958037#editor/target=post;postID=7269024980841579619), there is really little disagreement on the articulated goals of:
It is obvious that they do not differ from one another with regard to ends but only as to means. They all pretend to aim at the highest material welfare for the majority of citizens.
To me, the most important discussions should focus not on what we aim to achieve but instead on what is actually possible. Going all in aspiring to use the power of the state in order to strive toward a perfect world may sound good, but this experiment has been tried before. The product was not perfection but was instead perfectly awful. What limits our actions in regards to delivery of health care and specifically, what are the limits on state action? Why can't the state use the power of law to simply declare that health care is a right and that ALL those within the borders of the US should have access to health care?
Obviously entire books have been devoted to this and I will not exhaustively delve into all aspects of this question in this essay. The undisputed fact that so much has been and continues to be written belies the complexity involved. However, at the simplest level, you cannot mandate access to what you cannot define, particularly when the definition of what you are referring to is constantly morphing and evolving. Making something a legal right backed by the coercive power of the state requires that you must define the scope of that right. Decentralized private markets and charities are much more nimble in this regard. What one party does at any given time can be distinctly different from other parties involved in similar activities. This is not the case for legal rights. If one cannot define the nature of the right involved, it moves the action, however desirable at a theoretical basis, into the realm of practically impossible. Every decision regarding what is covered can be moved from the personal and medical into the legal realm. If you don't believe this will become unmanageable almost immediately, please refer to the case of Michelle Koselek in Massacheusettes (http://www.cbsnews.com/8301-201_162-57520960/mass-officials-to-fight-murderers-sex-change/).
The issues with defining the scope of any health care right was recently highlighted in the NEJM (http://www.nejm.org/doi/full/10.1056/NEJMp1208386)in a piece by Neuman and Chambers entitled "Medicare's Enduring Struggle to define Reasonable and Necessary Care". In the article the authors note:
Since its inception in 1965, Medicare policy has been guided by legislation mandating that the program not pay for items and services that are not “reasonable and necessary.” Over the years, amid escalating costs and the medical community's embrace of evidence-based medicine, the Centers for Medicare and Medicaid Services (CMS) has struggled to interpret and apply the “reasonable and necessary” criteria. At key junctures, CMS has been thwarted by political pressure or the courts. As Medicare spending takes center stage in the country's budget debates, “reasonable and necessary” warrants a closer look.
Neither necessary of reasonable is definable in any way meaningful way which will create any enduring structure which can address allocation of scarce resources. Neuman and Chambers dance around this issue and conclude by noting:
It may be tempting to believe that the matter will be rendered moot by payment reform and premium-support policies. That is, some may hope that the federal government can simply delegate coverage decisions to other parties, such as accountable care organizations, while forcing patients to consider the value of technologies through increased cost sharing. Such reforms are needed, since they will help move CMS out of the business of micromanaging coverage policy, though the details will be crucial. Offloading financial risk, however, does not absolve Medicare. Although it will shield CMS from certain controversies, questions will persist over how much geographic and socioeconomic variation in technology coverage the country will tolerate in a federal program. Moreover, the steady march of big-ticket, high-profile technology, such as cancer therapies, will demand a single response from Medicare regarding the adequacy and reasonableness of the evidence base.
Thus they admit that the creation of Medicare requires implementation of one size fits all approaches to defining scope. Where will those decisions be made? Whatever the initial intentions of those charged with defining and implementation will be co opted in the realm where all government decisions are made; the political realm. Political allocation of resources yields decisions which generate votes. The political realm works in a winner take all environment where those who can muster tiny majorities can impose their wills on substantial minorities, even if their governance may be unwise.
If the purpose of actions is to strive toward some ideal, whether effective or not, then aspiration alone can be a measure of success. However, I aim for more and am fearful of Utopian aspirations used to justify concentrations of power as a means to attempt what may be theoretically desirable but is almost certainly not attainable in the world of imperfect humans playing politics.
Saturday, November 10, 2012
The flaws of encounter based healthcare delivery
I am reading Lawrence and Lincoln Weed's book "Medicine in Denial". I became interested in this book after seeing a video of Dr. Lawrence Weed's Grand Rounds presentation at Emory University which dates back to the early 1970's. I blogged on this presentation earlier this year (http://georgiacontrarian.blogspot.com/2012/07/failure-of-our-intuition.html). Dr. Weed popularized the problem based medical record concept. His views on information collection, analysis, and use were far ahead of his time and concepts that he recognized 50 years ago are only now getting more widespread acceptance.

The concepts are really rather simple. Dr. Weed believes that everything starts with information collection and that to move rapidly toward decision making and action before a broad information collection effort is undertaken leads to disjointed and sub-optimal care. Dr. Weed divides the tasks into choice, collection, and analysis. I similarly divide the tasks into collection, analysis, and decision making and group the choice of which data to collect into the collection step while adding the decision making step which falls as a consequence of the analysis.

Under the current conditions, we attempt to cram everything into a very time constrained office visit. We might do some modest preoperative work ahead of time but for the most part, we experience our daily schedule of patient encounters as a series of agenda-less meetings. We walk in cold and start the process almost entirely from scratch, hurrying to collect relevant data, taking every shortcut imaginable to fast forward to diagnosis and plan implementation. We structure the encounter to limit the amount of any patient push back, with success being measured by how quickly we can get patients to accept our snap judgements and shoot from the hip plans. So much for shared decision making except in your concept of this is that you share your decision and the patient quickly accepts them.
Dr. Weed recognized that many of the functions now undertaken by physicians under hurried circumstances can be delegated to non-physicians under less time constrained conditions aided by software which drives more comprehensive data collection. The net result COULD be that we enter the encounter much better prepared without the need to engage in extensive data collection. With data collection for the most part done and the data presented in formats enhanced to facilitate analysis and decision making, the physician's job would be to facilitate decision making and implementation.

The key to deployment of this model is to put in place the data collection piece. In my own operating unit within a large "integrated" health care organization (and integrated is in quotes for a reason), we have made strides in moving toward collection of structured data in the clinical environments. However, the tools we use are still focused on office based encounters. The electronic tools which we are using which allow for the collection of structured data allow us to do this ONLY when we have the patient in the office. If we have an remote interaction and we place notes in the chart relating to this interaction, it is stored not as structured data but only as text blobs which can be mined for data only with great difficulty.
I suspect that our circumstances are not unique. The electronic medical record a still structured best as a billing justification tool, not a communication and performance improvement tool. It will be a huge waste of money if we spend billions of dollars to deploy a tool which locks us into bad workflow. Key to moving to efficient and less expensive care is offloading tasks such as data collection from expensive providers and moving activities from high cost environments such as hospitals and medical offices to where the patient are. If the only place our electronic tools allow us to collect key information is in high cost environments and that the tasks can only be done by high cost providers, we are sunk.
The concepts are really rather simple. Dr. Weed believes that everything starts with information collection and that to move rapidly toward decision making and action before a broad information collection effort is undertaken leads to disjointed and sub-optimal care. Dr. Weed divides the tasks into choice, collection, and analysis. I similarly divide the tasks into collection, analysis, and decision making and group the choice of which data to collect into the collection step while adding the decision making step which falls as a consequence of the analysis.
Under the current conditions, we attempt to cram everything into a very time constrained office visit. We might do some modest preoperative work ahead of time but for the most part, we experience our daily schedule of patient encounters as a series of agenda-less meetings. We walk in cold and start the process almost entirely from scratch, hurrying to collect relevant data, taking every shortcut imaginable to fast forward to diagnosis and plan implementation. We structure the encounter to limit the amount of any patient push back, with success being measured by how quickly we can get patients to accept our snap judgements and shoot from the hip plans. So much for shared decision making except in your concept of this is that you share your decision and the patient quickly accepts them.
Dr. Weed recognized that many of the functions now undertaken by physicians under hurried circumstances can be delegated to non-physicians under less time constrained conditions aided by software which drives more comprehensive data collection. The net result COULD be that we enter the encounter much better prepared without the need to engage in extensive data collection. With data collection for the most part done and the data presented in formats enhanced to facilitate analysis and decision making, the physician's job would be to facilitate decision making and implementation.
The key to deployment of this model is to put in place the data collection piece. In my own operating unit within a large "integrated" health care organization (and integrated is in quotes for a reason), we have made strides in moving toward collection of structured data in the clinical environments. However, the tools we use are still focused on office based encounters. The electronic tools which we are using which allow for the collection of structured data allow us to do this ONLY when we have the patient in the office. If we have an remote interaction and we place notes in the chart relating to this interaction, it is stored not as structured data but only as text blobs which can be mined for data only with great difficulty.
I suspect that our circumstances are not unique. The electronic medical record a still structured best as a billing justification tool, not a communication and performance improvement tool. It will be a huge waste of money if we spend billions of dollars to deploy a tool which locks us into bad workflow. Key to moving to efficient and less expensive care is offloading tasks such as data collection from expensive providers and moving activities from high cost environments such as hospitals and medical offices to where the patient are. If the only place our electronic tools allow us to collect key information is in high cost environments and that the tasks can only be done by high cost providers, we are sunk.
My blog sabbatical
I have been away from my blog. I can't say for sure why I have not been inspired to write. I suspect it has been a combination of factors: time, the election, Hurricane Sandy, and the natural cycle of writing.
I find politics both consuming and possibly irrelevant. Some much of what candidates say in the lead up to elections is really irrelevant to what they actually try to do or succeed in doing once elected. In many respects political leaders function within political systems very much like our individual conscious selves within our brains. Jonathan Haidt writes (in his book The Happiness Hypothesis) of a rider on a conscious rider on an unconscious elephant.

" I'm holding the reins in my hands, and by pulling one way or the other I can tell the elephant to turn, to stop, or to go. I can direct things, but only when the elephant doesn't have desires of his own. When the elephant really wants to do something, I'm no match for him.
...The controlled system [can be] seen as an advisor. It's a rider placed on the elephant's back to help the elephant make better choices. The rider can see farther into the future, and the rider can learn valuable information by talking to other riders or by reading maps, but the rider cannot order the elephant around against its will...
...The elephant, in contrast, is everything else. The elephant includes gut feelings, visceral reactions, emotions, and intuitions that comprise much of the automatic system. The elephant and the rider each have their own intelligence, and when they work together well they enable the unique brilliance of human beings. But they don't always work together well."
Under ideal circumstances, like the rider a political leader can lead by seeing into the future and help the electorate make better choices. However, it rarely works that way. The electorate generally fails to understand that political tools are very limited in terms of what issues can be effectively addressed. Political entities can pass laws which ostensibly can compel people to behave in certain ways. They also can take money from from one set of people and transfer it to another set of people. Neither of these tools are particularly precise and as political entities become more ambitious, the intended consequences tend to become dwarfed by the unintended consequences of their actions.
Still, people tend to overstate the capabilities of government to solve problems. The
issue is long standing. In the old testament in Samuel, the Israelites demand that they have a King. Basically everyone else had one and it was reasonable to believe that their problems could be more effectively addressed by allocating power to a single wise individual. However, concentrated power generally ends up in the hands of those who desire it most and more often than not, they are motivated primarily NOT by their desire for public service. Furthermore, even if they are fundamentally good, the elephant driver issue will render them less than optimally effective. The elephant will end up going where it wants to go short of actions which incapacitate the elephant. No one is a winner under those circumstances.
I think back upon my undergraduate days when I was friends with a Mr. John ___. He was part of a menagerie of very interesting and entertaining individuals all residing in my dormitory. It was a very different world whose most distinguishing feature was that its inhabitants still retained a very robust sense of humor. Most of us were not living our lives in an attempt to avoid any action which could affect our political careers 20 years in the future. We did things which now in retrospect might have required some degree of explanation on current applications for hospital credentials.
I believe it was during John's junior year that he decided to run for president of the the student body. He was a consummate outsider, not a member of Greek life unless one viewed him as an official member of GDI. We were a cynical bunch, cynical of politics are any level. The Watergate scandal was ongoing and there was skepticism that any of the scoundrels could be trusted. John came up with what I still believe was a brilliant idea. He would run on the apathy ticket and his slogan was to be "Don't vote. Elect John!". It was his plan to claim all the votes of students who failed to vote. His election platform was to dismantle student government and his mandate would come if less than half of the student body voted.

As it turned out, slightly more than half of the student body voted, thus undermining John's claim to higher office. However, the story was not so straight forward. For reasons not entirely clear, some of the students actually voted for John and if one to remove these votes from the total, less than half the student body actually voted. Legitimately John could claim that those who voted for him cost him the election! He was heart broken and I believe that this was his last foray into the quest for higher office.
I think John basically had it right. Be skeptical of the capabilities of what elected offices can accomplish. It is too bad that this message is so hard to translate into enlightened leadership that understands its limits. You can be undermined even by those who are trying to help.
I find politics both consuming and possibly irrelevant. Some much of what candidates say in the lead up to elections is really irrelevant to what they actually try to do or succeed in doing once elected. In many respects political leaders function within political systems very much like our individual conscious selves within our brains. Jonathan Haidt writes (in his book The Happiness Hypothesis) of a rider on a conscious rider on an unconscious elephant.
" I'm holding the reins in my hands, and by pulling one way or the other I can tell the elephant to turn, to stop, or to go. I can direct things, but only when the elephant doesn't have desires of his own. When the elephant really wants to do something, I'm no match for him.
...The controlled system [can be] seen as an advisor. It's a rider placed on the elephant's back to help the elephant make better choices. The rider can see farther into the future, and the rider can learn valuable information by talking to other riders or by reading maps, but the rider cannot order the elephant around against its will...
...The elephant, in contrast, is everything else. The elephant includes gut feelings, visceral reactions, emotions, and intuitions that comprise much of the automatic system. The elephant and the rider each have their own intelligence, and when they work together well they enable the unique brilliance of human beings. But they don't always work together well."
Under ideal circumstances, like the rider a political leader can lead by seeing into the future and help the electorate make better choices. However, it rarely works that way. The electorate generally fails to understand that political tools are very limited in terms of what issues can be effectively addressed. Political entities can pass laws which ostensibly can compel people to behave in certain ways. They also can take money from from one set of people and transfer it to another set of people. Neither of these tools are particularly precise and as political entities become more ambitious, the intended consequences tend to become dwarfed by the unintended consequences of their actions.
Still, people tend to overstate the capabilities of government to solve problems. The
issue is long standing. In the old testament in Samuel, the Israelites demand that they have a King. Basically everyone else had one and it was reasonable to believe that their problems could be more effectively addressed by allocating power to a single wise individual. However, concentrated power generally ends up in the hands of those who desire it most and more often than not, they are motivated primarily NOT by their desire for public service. Furthermore, even if they are fundamentally good, the elephant driver issue will render them less than optimally effective. The elephant will end up going where it wants to go short of actions which incapacitate the elephant. No one is a winner under those circumstances.
I think back upon my undergraduate days when I was friends with a Mr. John ___. He was part of a menagerie of very interesting and entertaining individuals all residing in my dormitory. It was a very different world whose most distinguishing feature was that its inhabitants still retained a very robust sense of humor. Most of us were not living our lives in an attempt to avoid any action which could affect our political careers 20 years in the future. We did things which now in retrospect might have required some degree of explanation on current applications for hospital credentials.
I believe it was during John's junior year that he decided to run for president of the the student body. He was a consummate outsider, not a member of Greek life unless one viewed him as an official member of GDI. We were a cynical bunch, cynical of politics are any level. The Watergate scandal was ongoing and there was skepticism that any of the scoundrels could be trusted. John came up with what I still believe was a brilliant idea. He would run on the apathy ticket and his slogan was to be "Don't vote. Elect John!". It was his plan to claim all the votes of students who failed to vote. His election platform was to dismantle student government and his mandate would come if less than half of the student body voted.
As it turned out, slightly more than half of the student body voted, thus undermining John's claim to higher office. However, the story was not so straight forward. For reasons not entirely clear, some of the students actually voted for John and if one to remove these votes from the total, less than half the student body actually voted. Legitimately John could claim that those who voted for him cost him the election! He was heart broken and I believe that this was his last foray into the quest for higher office.
I think John basically had it right. Be skeptical of the capabilities of what elected offices can accomplish. It is too bad that this message is so hard to translate into enlightened leadership that understands its limits. You can be undermined even by those who are trying to help.
Sunday, October 21, 2012
Placing the taxing power in the hands of public health maximizers
There is a provocative piece published in the NEJM entitled "The taxing power and the Public's health" (http://www.nejm.org/doi/full/10.1056/NEJMp1209648?query=featured_home). It takes a different tack on the Supreme Court's decision to call the health insurance mandate a tax and the implications of this decision for future use of the taxing tool to promote public health. The authors find the use of
taxes as a nudge appealing:
I find the concept very disturbing, not because I am not interested in public health, but because of the tendency for such actions to move from a constrained realm to an uncontrolled one. I am reminded of the work of Dr. Barry Schwarz, author of "The paradox of choice", who identified tendencies in all of us to function as "maximaizers" or "sufficers". Maximizers tend to refuse to settle for choices which they perceive as yielding results which could be better. Sufficers are OK with approaches and decisions which yield results which meet their ends. Coercive tools in the hands of sufficers are less likely to result in problems. Place those tools in the hands of maximizers and there will be no end to to coercive madness set in motion, all in the name of improving public health.
It all hinges on the vision of what one believes that coercive public health powers placed in the hands of zealots can and should do. It is really no different from the broader view of the role of voluntary vs. coercive tools to mold, influence, and alter human behavior. I for one view that the widespread deployment of taxing tools to "nudge" people should viewed with great prejudice. The default mode should be to allow the greatest degrees of human freedom and to implement coercive tools, whether legal or financial sanctions, as infrequently as possible.

While those championing use of taxing power to change human behavior may be motivated by the highest of motivations and believe they are furthering public good, the powers they unleash will almost certainly be exploited by those who motivations are not so noble.
taxes as a nudge appealing:
Taxes are an appealing mechanism of public health regulation for several reasons. They proffer “nudges” and market-based solutions as alternatives to rigid mandates. Tax-based policies like the SRP retain an element of voluntariness, especially since lawmakers can calibrate the tax penalty to the importance of the desired behavior change. There’s strong evidence that taxes affect consumption decisions. Finally, tax strategies are “win–win” for governments, either leading people to take health-enhancing steps or collecting revenue to fund health or other programs.
I find the concept very disturbing, not because I am not interested in public health, but because of the tendency for such actions to move from a constrained realm to an uncontrolled one. I am reminded of the work of Dr. Barry Schwarz, author of "The paradox of choice", who identified tendencies in all of us to function as "maximaizers" or "sufficers". Maximizers tend to refuse to settle for choices which they perceive as yielding results which could be better. Sufficers are OK with approaches and decisions which yield results which meet their ends. Coercive tools in the hands of sufficers are less likely to result in problems. Place those tools in the hands of maximizers and there will be no end to to coercive madness set in motion, all in the name of improving public health.
It all hinges on the vision of what one believes that coercive public health powers placed in the hands of zealots can and should do. It is really no different from the broader view of the role of voluntary vs. coercive tools to mold, influence, and alter human behavior. I for one view that the widespread deployment of taxing tools to "nudge" people should viewed with great prejudice. The default mode should be to allow the greatest degrees of human freedom and to implement coercive tools, whether legal or financial sanctions, as infrequently as possible.
While those championing use of taxing power to change human behavior may be motivated by the highest of motivations and believe they are furthering public good, the powers they unleash will almost certainly be exploited by those who motivations are not so noble.
Sunday, September 30, 2012
Online dating as a model for health care outcomes research
I heard an interview with Dan Ariely while listening to CNBC today. He is one of my favorite authors but I was not aware of his work done focusing on online dating services. What struck me about his work and comments was the nature of the critique; online dating services may be of limited value because they collect the wrong data. They collect data that is easily defined and relatively easy to collect such as income, education, height, and weight. Based upon the information presented, users of these services appear to be remarkably superficial in terms of what they value. However, they may be superficial because of the information presented to them.
I was struck by the parallels to current state of outcomes research efforts in health care. We tend to focus on measures which often are process measures or outcomes measures which are at best proxies to something more important. We use administrative databases because they are the only sources of structured data we might have access to. We do so because in the absence of robust things to measure, we end up collecting data on what we can collect and measuring what is measurable.
Ariely talks about collecting match-making questionnaires on a variety of people, some of whom he liked and others from those he did not care for. He then reviewed the blinded questionnaires and attempted to sort out from these data whether he could discern whether he could tell those which came from the people he had a personal affinity for vs. those he did not click with. He could not. Thus the information collected was not helpful in predicting personal chemistry. In the same sense I would predict that the current state of data collection and analysis used for assessing outcomes and quality will suffer from similar issues. By focusing on what we can measure, we are likely to focus on things that are not particularly important in the delivery of health care.
I think the lesson is not that we should not strive to collect data to drive practice change. We just need to be VERY circumspect about what we strive to collect and how we use it. Our processes focusing on performance improvement also need to be a focus of performance improvement.
Sunday, September 23, 2012
Retirement as an entitlement
When we solely operated as family units, almost involvement was needed to meet the needs of individual members and the group. There was no such thing as retirement. As family members became infirmed, their engagement was limited because they could not bring much to the table. As social systems became more complex, obligations of single individuals to others also became more complex. Some relationships like those binding close family remained in the informal realm while increasingly our relationships to other and the attendant obligations fell increasingly into the legal realm. However the obligations were defined and enforced, the well being of those involved depended upon the existence of adequate resources to meet essential human needs. There had to be enough food, shelter, fuel, and water for all to survive. Until very recently having a portion of one's life set aside without the requirement to create or gather essential resources was only a pipe dream.
I believe the problem we have is one of disbelief and perception. We have grown up in such a world of plenty that we simply cannot imagine that our individual withdrawal from the workforce could possibly mean that we will have any effect on what is available to meet human needs. Thus, of course we should be able to retire at aged 65. Why not 55 or even 50? Why should I not have access to all this plenty, even if I do not contribute in any material way to its existence? What better entity that government to protect those who cannot protect themselves. Who could have foreseen that extension of those same protections to a larger and not so vulnerable audience would become the perfect tool to win elections.
The reality is retirement is a new concept and the selection of the age of 65 was random event based upon the life expectancy over 80 years ago. Promises were made when Social Security was founded that are now actuarial fantasy. Pension systems were created by companies based upon the same bad assumptions. They either figured out how to extricate themselves from those promises or they went bankrupt. How Darwnian!
Saturday, September 22, 2012
A trickle down idea from a rich 1% Democrat
Strictly defined, Private Health isn't part of the growing phenomenon known as concierge medicine, where doctors charge a retainer for more face-time and personal attention, and often take their practices off the commercial and government payment grid. Private Health isn't an insurance company either and maintains no contractual or financial relationship with its doctors. "We don't buy access," Mr. Michelson says. A large part of what Private Health does is simply match patients with physicians, which isn't as obvious as it sounds. "People do not know how to choose doctors. It's one of the most important things you can do to promote your own health and that of your loved ones, and it's: 'My friend's cousin's relative went to Dr. Smith, and he was terrific.' Well, how do you know he's terrific?" So Mr. Michelson built a series of proprietary algorithms to distinguish "the few who are the very best" from "the many who are very good," based on "the factors that predict excellence."However, I think the key statement comes somewhat later in the interview:
"As the biomedical revolution took off," Mr. Michelson says, "there should have been a counterbalance of somebody taking the position of the general contractor, the manager, and investing in the systems, the technologies and the processes to keep up." But the organization of medicine as an industry didn't change. So the health-care delivery system, to the extent it qualifies as a system, "has no quality control, no integration, no coordination." Doctors "tend to operate in an independent and isolated way, and even specialists who've been treating the same patient for years and years typically never, ever speak to one another."http://online.wsj.com/article/SB10000872396390444620104578008182459803120.html?mod=WSJ_Opinion_LEADTop
The business plan of Private Health Management is to basically supply an uncovered service to people who can pay for it. In that sense it is similar to concierge care or provision of lasik surgery or botox injections. The bad news it is not covered by insurance. However, the good news is that it is outside the constraints of the present day third party payment system. I would say the trade off is more than worth it if you can come up with the dough.
The sad truth is that despite all of the talk about rewarding coordination of care, there is no explicit and consistent payment of time devoted to such activities within the current payment structure. There may be a few ongoing experiments which are likely to disappear when their grants dry up. If the public were to wait for the current players in health to development of such a key element of care, it would never happen. As a precondition for development, the mainstream players would insist it develop as part of the current payment system. I am afraid that it would quickly be co opted by those who fare well under the current payment structure which rewards expensive and fragmented care.

Ultimately, for optimal care the care coordination piece must be embedded locally. Someone needs to be in charge. Someone other than the patient or their family needs to be the general contractor.
Sunday, September 16, 2012
Help prevent blindness
I have learned much by being a dog owner. Today we are celebrating the birthday of our older hound who is the best dog in the world. She is 17 years old today, a remarkable feat for a chocolate lab. They are not supposed to live this long. Her mother died before age 10 and she has outlived everyone in her litter. Before the ravages of age caught up with her she was a remarkable athlete, with the best snout-eye coordination I have ever seen. Her disposition was close to perfect. I have thought about the utility of having her exome sequenced. If there is a genetic basis for such a perfect animal, then we should have this data.
 However, she is now 17 years old and as far as we can tell she can still smell but she is virtually blind and completely deaf. She can sense her world only by sniffing it and running into it. Her present state of being does not allow her to see what is coming, except in very narrow circumstances. Even then she finds herself running into things and if we did not put up barriers and guide her, she would end up falling down stairs. Loss of key senses prevents her from anticipating and avoiding hazards.
However, she is now 17 years old and as far as we can tell she can still smell but she is virtually blind and completely deaf. She can sense her world only by sniffing it and running into it. Her present state of being does not allow her to see what is coming, except in very narrow circumstances. Even then she finds herself running into things and if we did not put up barriers and guide her, she would end up falling down stairs. Loss of key senses prevents her from anticipating and avoiding hazards.
 It is essential for all living beings to have such an ability and to use it wisely. In the same sense, such functionality also extends to entities which are formed by the actions of groups of people. Organizations which are blind to how their actions in the present impact their group in the future are destined to do things which will result in actions which will result in bad consequences. Individuals who belong to organizations have eyes and ears, but these are no the sensory organs which directly guide these entities. These organizations receive feedback in the form of membership numbers, dues, contributions, and recognition. Like living beings these entities require food and ego gratification. Money serves as the fuel that feeds their energy needs and recognition provides the ego gratification. In a sense, financial tools represent sensory organs for organizations. Money is like the photons which shed light on the structures which an organization has in place to make sure it is viable.
It is essential for all living beings to have such an ability and to use it wisely. In the same sense, such functionality also extends to entities which are formed by the actions of groups of people. Organizations which are blind to how their actions in the present impact their group in the future are destined to do things which will result in actions which will result in bad consequences. Individuals who belong to organizations have eyes and ears, but these are no the sensory organs which directly guide these entities. These organizations receive feedback in the form of membership numbers, dues, contributions, and recognition. Like living beings these entities require food and ego gratification. Money serves as the fuel that feeds their energy needs and recognition provides the ego gratification. In a sense, financial tools represent sensory organs for organizations. Money is like the photons which shed light on the structures which an organization has in place to make sure it is viable.
Democratically formed states represent a special form of organizational entity. Where voluntary organizations are completely dependent upon serving their membership, political states are different. If members become blind to the wants and desires of their members or those who provide financial resources, the members will leave and the donors will stop donating. Blindness is a death sentence. In contrast, political entities have the ability to compel people to continue to feed them whether they are blind to their constituent needs or not.
If a private entity cannot meet its payroll needs, the world is generally not so forgiving. The message will be sent, find a way to convince others to voluntarily provide your organization with financial resources you need or cease to exist. A public entity supported by taxes can ignore such signals, at least for a while.
This may have its merits. Government support of basic research is justified based upon the lack of support that would be forthcoming from private sources. This might be true but the issue becomes once the genie is out of the bottle how do political entities create boundaries which they do not cross? How can they say no? Absent the usual financial sensory organs which maintain discipline for private entities, once states start down a given path, how do they know where they are going to end up if they are flying blind?
 When my blind dog walks around, she gets feedback whenever she walks into something. I suspect that is a painful experience and she cannot continue because something is in her way. We structure her environment such that we avoid existential threats such as falling down a flight of stairs or walking off a cliff. How do governments, blindly operating without the usual financial vision avoid existential threats? I am not sure we have an answer to this question. It is not impossible to deploy the same financial tools to state entities as we apply to private entities.
When my blind dog walks around, she gets feedback whenever she walks into something. I suspect that is a painful experience and she cannot continue because something is in her way. We structure her environment such that we avoid existential threats such as falling down a flight of stairs or walking off a cliff. How do governments, blindly operating without the usual financial vision avoid existential threats? I am not sure we have an answer to this question. It is not impossible to deploy the same financial tools to state entities as we apply to private entities.

The barriers to deployment are political. Being or appearing to be blind to financial reality confers a short term political advantage to those running for office. That is actually a very frightening thought in that we now operate in a system that provides leadership with an incentive to be blind. I look at my old blind dog and see what blindness means to her. She has benevolent owners who keep her from walking off a cliff. When our leadership cultivates blindness, who will prevent us from walking off a similar cliff.
Democratically formed states represent a special form of organizational entity. Where voluntary organizations are completely dependent upon serving their membership, political states are different. If members become blind to the wants and desires of their members or those who provide financial resources, the members will leave and the donors will stop donating. Blindness is a death sentence. In contrast, political entities have the ability to compel people to continue to feed them whether they are blind to their constituent needs or not.
If a private entity cannot meet its payroll needs, the world is generally not so forgiving. The message will be sent, find a way to convince others to voluntarily provide your organization with financial resources you need or cease to exist. A public entity supported by taxes can ignore such signals, at least for a while.
This may have its merits. Government support of basic research is justified based upon the lack of support that would be forthcoming from private sources. This might be true but the issue becomes once the genie is out of the bottle how do political entities create boundaries which they do not cross? How can they say no? Absent the usual financial sensory organs which maintain discipline for private entities, once states start down a given path, how do they know where they are going to end up if they are flying blind?
The barriers to deployment are political. Being or appearing to be blind to financial reality confers a short term political advantage to those running for office. That is actually a very frightening thought in that we now operate in a system that provides leadership with an incentive to be blind. I look at my old blind dog and see what blindness means to her. She has benevolent owners who keep her from walking off a cliff. When our leadership cultivates blindness, who will prevent us from walking off a similar cliff.
Saturday, September 8, 2012
Emotional decision making, fear, and muda
There is no question that fear acts as a huge motivational factor for people in general. Our perception of risk is mediated by our emotional and cognitive brains, but the readout of fear tends to be primarily emotional, often leading to irrational decisions, both by individuals and institutions. The logical sequences goes as follows:

1. Bad event happens and instills fear broadly
2. Causality is inferred from coincidental events
3. A broad response is implemented irregardless of any evidence to the contrary, irregardless of evidence supporting effectiveness, and without any mechanisms to assess effectiveness in the future
4. We are saddled with muda. You might ask what muda is. It is a Japanese term denoted activity denoting activity with no discernible value. It is waste.
In today's WSJ, Simons and Chabris wrote an essay "Do our gadgets really threaten planes?" I have often wondered why we a forced to turn off our electrical devices during takeoff and landing. It was hard to conceive that my kindle reader could conceivably cause a problem but I comply with the requests. I carry some sort of paper alternative to keep me occupied during those windows of time. Simons and Chabris give some historical perspective on these restrictions which turn out to be based upon a few isolated reports of pilots and flight crews who believed that passenger gadgets disrupted navigational and/or flight communication systems. No one has been able to duplicate these observations.

Furthermore, the authors own statistical analysis based upon passenger survey data and compliance with regulations (or lack thereof) really call into question that these particular regulations create any sort of benefit for anyone. It turns out that 40% of passengers did not turn phones off completely, 7% left them on with full WiFi and cellular activity, and 2% pulled what they referred to as a "full Baldwin", continuing to use their phones actively. If their sample is representative, we can assume that personal electronic devices are operational on virtually all flights and we should see some sort of disruption of flight functions if there is a real risk. We have not observed this. Yet the restrictions persist, based upon the precautionary principle. The default mode is to avoid or prohibit activities where there is a perception that some harm may follow, irregardless of evidence or lack thereof.
 This article struck a chord because we engage in this type of thinking in medicine. I have touched upon this in a previous blog (http://georgiacontrarian.blogspot.com/2010/10/anecdote-driven-activity.html). At least part of the problem is our default to the precautionary principle, that no matter how remote the possibility, any scenario where a very bad outcome is at all possible requires some sort of action, even if the action is of unproven benefit. Despite the technological advances in medicine over the pat century, it is my experience that those who practice the healing arts tend not to think of things in quantitative terms. Part of the problem is the lack of actual quantitative data.
This article struck a chord because we engage in this type of thinking in medicine. I have touched upon this in a previous blog (http://georgiacontrarian.blogspot.com/2010/10/anecdote-driven-activity.html). At least part of the problem is our default to the precautionary principle, that no matter how remote the possibility, any scenario where a very bad outcome is at all possible requires some sort of action, even if the action is of unproven benefit. Despite the technological advances in medicine over the pat century, it is my experience that those who practice the healing arts tend not to think of things in quantitative terms. Part of the problem is the lack of actual quantitative data.
An additional aspect is that available data provides a picture which is not so black and white. I have discussed these elements with previous posts. (http://georgiacontrarian.blogspot.com/2010/09/framing-issues-and-informed-consent.html http://georgiacontrarian.blogspot.com/2011/02/what-is-right-answer-framing-and.html). Understanding and communicating risks is easy if the choices are stark. Choices are rarely so, but time constraints tend to drive us to make the choices appear stark, even when they are not. Over time it becomes convenient for us has health care providers to embrace the starkness of the options as well. It simplifies our lives in the short term but we end up is strange and undesirable places because we end up recommending all sorts of wasteful interventions based upon precautionary principles. Over time there are inexorable pressures to implement such interventions under increasing mundane circumstances, often driven by random anecdote or extraordinarily unlikely outcomes. The irony is the process is so gradual and the incentives so perverse that we end up being completely comfortable with trying to defend positions which may appear to be embarrassingly indefensible. I suspect that this may have been the case with physicians whose actions end up crossing legal lines. (http://georgiacontrarian.blogspot.com/2011/06/radio-fence-principle.html)
 There are all sorts of estimates as to how much of health care dollars are wasted. Unfortunately, this too is nuanced and not simple arithmetic. Whether what I describe above falls into the bucket of defensive medicine or something else and whether the influence of such thinking can be quantitative or not is an open question. From my perspective as a practicing physician I perceive this cognitive issue has profound financial impact and this issue cannot be addressed until we can address a cultural divide which needs to be bridged. Practicing physicians tend to be hostile to those who attempt to guide practice based upon quantitative data as evidenced by the reception that the USPSTF receives when they make recommendations that call into question widespread screening practices.
There are all sorts of estimates as to how much of health care dollars are wasted. Unfortunately, this too is nuanced and not simple arithmetic. Whether what I describe above falls into the bucket of defensive medicine or something else and whether the influence of such thinking can be quantitative or not is an open question. From my perspective as a practicing physician I perceive this cognitive issue has profound financial impact and this issue cannot be addressed until we can address a cultural divide which needs to be bridged. Practicing physicians tend to be hostile to those who attempt to guide practice based upon quantitative data as evidenced by the reception that the USPSTF receives when they make recommendations that call into question widespread screening practices.
 We just can't help ourselves. Our decision making tools still rely on ancient hardware with emotional readouts that were extremely useful to our ancestors down by the watering hole which were essential when we needed to integrate the constellation of data in a hurry and tell us to run like hell. Even physicians who are schooled in numbers and outcomes recognize that this is part of clinical practice and decision making. (http://www.nejm.org/doi/full/10.1056/NEJMp1102632) However, we need to recognize this for what it is and be able to reflect in such a way that we can avoid the worst of the muda created.
We just can't help ourselves. Our decision making tools still rely on ancient hardware with emotional readouts that were extremely useful to our ancestors down by the watering hole which were essential when we needed to integrate the constellation of data in a hurry and tell us to run like hell. Even physicians who are schooled in numbers and outcomes recognize that this is part of clinical practice and decision making. (http://www.nejm.org/doi/full/10.1056/NEJMp1102632) However, we need to recognize this for what it is and be able to reflect in such a way that we can avoid the worst of the muda created.
1. Bad event happens and instills fear broadly
2. Causality is inferred from coincidental events
3. A broad response is implemented irregardless of any evidence to the contrary, irregardless of evidence supporting effectiveness, and without any mechanisms to assess effectiveness in the future
4. We are saddled with muda. You might ask what muda is. It is a Japanese term denoted activity denoting activity with no discernible value. It is waste.
In today's WSJ, Simons and Chabris wrote an essay "Do our gadgets really threaten planes?" I have often wondered why we a forced to turn off our electrical devices during takeoff and landing. It was hard to conceive that my kindle reader could conceivably cause a problem but I comply with the requests. I carry some sort of paper alternative to keep me occupied during those windows of time. Simons and Chabris give some historical perspective on these restrictions which turn out to be based upon a few isolated reports of pilots and flight crews who believed that passenger gadgets disrupted navigational and/or flight communication systems. No one has been able to duplicate these observations.
Furthermore, the authors own statistical analysis based upon passenger survey data and compliance with regulations (or lack thereof) really call into question that these particular regulations create any sort of benefit for anyone. It turns out that 40% of passengers did not turn phones off completely, 7% left them on with full WiFi and cellular activity, and 2% pulled what they referred to as a "full Baldwin", continuing to use their phones actively. If their sample is representative, we can assume that personal electronic devices are operational on virtually all flights and we should see some sort of disruption of flight functions if there is a real risk. We have not observed this. Yet the restrictions persist, based upon the precautionary principle. The default mode is to avoid or prohibit activities where there is a perception that some harm may follow, irregardless of evidence or lack thereof.
An additional aspect is that available data provides a picture which is not so black and white. I have discussed these elements with previous posts. (http://georgiacontrarian.blogspot.com/2010/09/framing-issues-and-informed-consent.html http://georgiacontrarian.blogspot.com/2011/02/what-is-right-answer-framing-and.html). Understanding and communicating risks is easy if the choices are stark. Choices are rarely so, but time constraints tend to drive us to make the choices appear stark, even when they are not. Over time it becomes convenient for us has health care providers to embrace the starkness of the options as well. It simplifies our lives in the short term but we end up is strange and undesirable places because we end up recommending all sorts of wasteful interventions based upon precautionary principles. Over time there are inexorable pressures to implement such interventions under increasing mundane circumstances, often driven by random anecdote or extraordinarily unlikely outcomes. The irony is the process is so gradual and the incentives so perverse that we end up being completely comfortable with trying to defend positions which may appear to be embarrassingly indefensible. I suspect that this may have been the case with physicians whose actions end up crossing legal lines. (http://georgiacontrarian.blogspot.com/2011/06/radio-fence-principle.html)
 There are all sorts of estimates as to how much of health care dollars are wasted. Unfortunately, this too is nuanced and not simple arithmetic. Whether what I describe above falls into the bucket of defensive medicine or something else and whether the influence of such thinking can be quantitative or not is an open question. From my perspective as a practicing physician I perceive this cognitive issue has profound financial impact and this issue cannot be addressed until we can address a cultural divide which needs to be bridged. Practicing physicians tend to be hostile to those who attempt to guide practice based upon quantitative data as evidenced by the reception that the USPSTF receives when they make recommendations that call into question widespread screening practices.
There are all sorts of estimates as to how much of health care dollars are wasted. Unfortunately, this too is nuanced and not simple arithmetic. Whether what I describe above falls into the bucket of defensive medicine or something else and whether the influence of such thinking can be quantitative or not is an open question. From my perspective as a practicing physician I perceive this cognitive issue has profound financial impact and this issue cannot be addressed until we can address a cultural divide which needs to be bridged. Practicing physicians tend to be hostile to those who attempt to guide practice based upon quantitative data as evidenced by the reception that the USPSTF receives when they make recommendations that call into question widespread screening practices.Thursday, September 6, 2012
Defining the health care "right"
This story does not require much comment. A convicted murderer in Massachusetts has successfully won a lawsuit gaining him access to transgender surgery. http://blogs.wsj.com/law/2012/09/04/judge-orders-sex-change-operation-for-federal-prisoner/ The judge in the suit wrote:
Judge Wolf, describing his 126-page order as “unprecedented,” said that denying Kosilek the surgery was a violation of the Eighth Amendment’s prohibition on cruel and unusual punishment.From the standpoint of defining limits on positive rights, this case essentially declares there are none. I simply cannot imagine that this will not be overturned. If this goes to the highest court in the land and is upheld, there is essentially nothing that cannot be successfully sued for in court in the health care arena. What additional medical interventions can those incarcerated with lots of time to think about gaming the system come up with? I can only imagine....
Sunday, September 2, 2012
One man's ideas are another man's ideology

Similarly, Maureen Dowd wrote today:
Again, there is the implication that no one could actually hold an world view different from Ms. Dowd. The only explanation is that the RNC engaged in some sort of elaborate hoax and deception of the American public.That’s why they knocked themselves out producing a convention that was a colossal hoax. They did that for us. Because they care. With exquisite timing, they started caring last Tuesday at 7 p.m., when suddenly the party was chockablock with tender souls in rainbow colors, with strong-minded women and softhearted men, with sentimental rags-to-riches immigrant sagas. We all know Republicans prefer riches-to-riches sagas and rounding up immigrants, if the parasitic scofflaws aren’t sensitive enough to self-deport. That’s why my heart swells to think of the herculean effort the G.O.P. put into pretending its heart bleeds.
The second assumption is:
All other ideologies, in approving of the search for the necessities of life, are forced in some measure to take into account the fact that division of labor is more productive than isolated work. They thus admit the need for social cooperation.The implication of this assumption is that incentives which affect cooperation are important. He goes on to say:
In fact, for all parties committed to pursuit of the people’s welfare and thus approving social cooperation, questions of social organization and the conduct of social action are not problems of ultimate principles and of world views, but ideological issues. They are technical problems with regard to which some arrangement is always possible. No party would wittingly prefer social disintegration, anarchy, and a return to primitive barbarism to a solution which must be bought at the price of the sacrifice of some ideological points.While this piece was written more than half a century ago and the terminology has evolved, the themes are consistent:
The accomplishment of improvement of material welfare is described by Mises as (bold is my emphasis):In the field of society’s economic organization there are the liberals advocating private ownership of the means of production, the socialists advocating public ownership of the means of production, and the interventionists advocating a third system which, they contend, is as far from socialism as it is from capitalism. In the clash of these parties there is again much talk about basic philosophical issues. People speak of true liberty, equality, social justice, the rights of the individual, community, solidarity, and humanitarianism. But each party is intent upon proving by ratiocination and by referring to historical experience that only the system it recommends will make the citizens prosperous and satisfied. They tell the people that realization of their program will raise the standard of living to a higher level than realization of any other party’s program. They insist upon the expediency of their plans and upon their utility. It is obvious that they do not differ from one another with regard to ends but only as to means. They all pretend to aim at the highest material welfare for the majority of citizens.
The problems involved are purely intellectual and must be dealt with as such. It is disastrous to shift them to the moral sphere and to dispose of supporters of opposite ideologies by calling them villains. It is vain to insist that what we are aiming at is good and what our adversaries want is bad. The question to be solved is precisely what is to be considered as good and what as bad. The rigid dogmatism peculiar to religious groups and to Marxism results only in irreconcilable conflict. It condemns beforehand all dissenters as evildoers, it calls into question their good faith, it asks them to surrender unconditionally. No social cooperation is possible where such an attitude prevails.I highlighted Dowd and Krugman only because the timing of the Republican convention. I am certain that the same behavior will be exhibited when Republican leaning columnists have their chance with the Democratic convention. Those who hold beliefs as to how improve the material well being of others which are different from ones you might believe are not necessarily evil or dishonest. However, from the perspective of exploiting differences in belief systems within the political realm, if is almost always more successful to take such a tack if in order to get elected.
This underscores an inherent issue with moving social problems into a the political realm. We may hold different views as to how the world works based upon differences in belief systems. Many if not most of the differences are based upon some empiric evidence, selectively embraced to support what we believe to be true. When these belief systems reside in the private domain, we are free to embrace what we chose to embrace and reap the rewards or suffer the consequences personally. There may be some spillover effects but as long as those who hold particular belief systems do not capture the coercive power of the state, most individuals will be free to embrace what they hold to be true and have their actions guided by them. There are limits to actions of individuals and for a review of this I recommend Richard Epstein's book, "Simple rules for a compelx world".
If the effects of state actions were unambiguous and apparent within the time frame of elections, this would not be such an issue. However, within the common election cycle of 2-4 years, assessment of actions within the political realm yield conflicting results. Ideas as to optimal rules and structures are difficult to test at best and assessments as to the wisdom of particular approaches may require decades to become apparent. Short term expediencies required to garner votes may capture the electorate but result in disastrous longer term outcomes. Similarly, vilifying those who disagree with us may be helpful to get elected but is dysfunctional when we need to create institutions which foster cooperation and coordination.
I believe that political processes are essentially incapable of accomplishing this on a consistent basis and for this reason the role of the state in human affairs needs to be limited. This idea dates back at least to the founding of our Republic. Whether it is true is a legitimate point for discussion. It is not desirable to vilify those those who hold this belief, to always question their motives, to call them frauds or perpetrators or hoaxes, of call them as crazy. It might get you elected but it will not improve the lives of your fellow citizens. We are all dependent on each other to survive and thrive and we can get to a better place when more of us are rowing in the same direction. That will happen when people voluntarily chose their path, not when someone else tries to force them.
Subscribe to:
Comments (Atom)