
I have been introduced to an interesting concept, that of co-production. I came upon this concept when I read an article published in BMJ Quality and Safety. (Link) It is actually such an intuitive concept that it is hard to imagine why it did not occur to me and everyone else previously. I guess that is just how ideas are.
In manufacturing, those who produce goods such as cars or consumables do not directly rely on those use consume and use those products to produce them. The end users may influence the characteristics of the products but they play little or no role in product manufacture. Consumers do not play a substantial role in the quality of the final product, whether that be automobiles or chicken pot pies.
The service industry is different. Victor Fuchs noted in 1968 that the new service economy was different from the old manufacturing economy in that the producers and consumers of services worked together to create value. Later Alfred Toffler described the next generation of consumers which he referred to as "prosumers", linking the previously separated function of production and consumption to maximize consumer value and minimize producer cost.
For example, one might hire a financial professional to help with retirement planning. No matter how good the advice of the professional, the final product depends upon the consumer. If the consumer does not follow the advice and put away money for the future, the final product will be substandard, no matter how good the advice. Similarly, if one gives your tax professional the wrong data, the final product of the tax return will not be up to snuff.
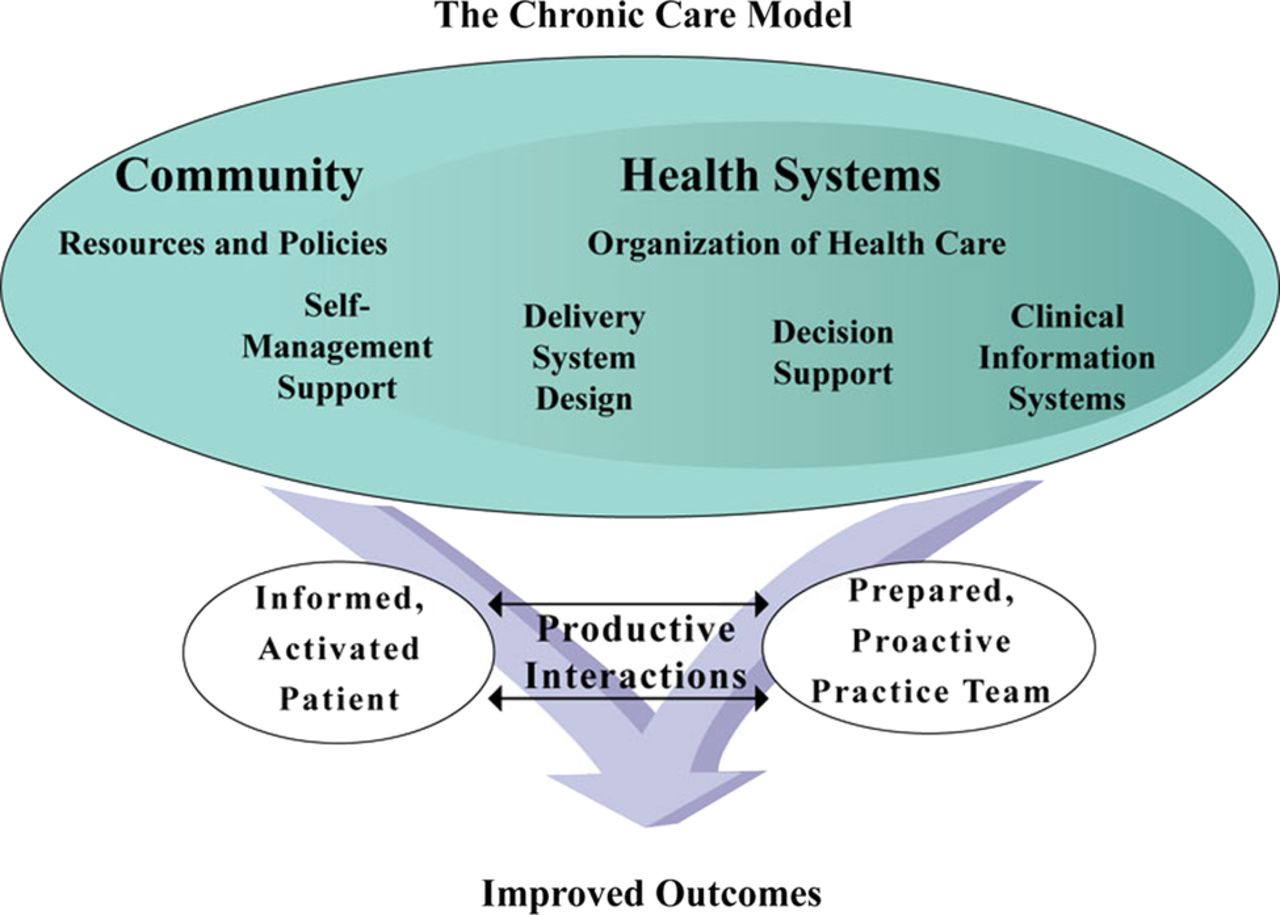
This concept is also very appropriate for many aspects health care delivery. For patients who present with a diagnostic problem, if they are not capable or willing to provide accurate or complete histories or reviews of systems, they are much less likely to receive accurate diagnoses. For patients who undergo surgery or other interventions who are then discharged home, if they are not willing or capable of following care instructions (or have not been appropriately educated), the outcomes of the interventions are much less likely to be favorable. For patients with chronic disorders where most of the care happens at home, their contributions and buy in may be most essential to optimal outcomes.
However, the co-production involves not just a given provider and a given patient, but teams of providers and other teams which may include patients, their families, and perhaps other patients.
How do we get better outcomes? You have to first figure out what you are trying to produce and then figure out who are the key players in co-producing the desired outcomes. This is going to take some major culture change, in both patients and professionals with health care delivery.
No comments:
Post a Comment