
The recent spate of reported mass killings perpetrated by maladjusted young men has raised all sorts of issues and various constituencies are clamoring for some sort of action. The action called for and the wisdom of any given intervention hinges on this whole issue of causality. Obviously, guns are the root cause these tragedies; we must ban guns. No, guns do not cause these events; there is a breakdown of morals or the family or desensitization to violence mediated by the overall coarsening of the media. We must address these issues.... and so on. It all hinges on understanding causality and when events are low frequency events, causality becomes almost impossible to dissect.
I saw a patient in the hospital today who was admitted because of a severe adverse drug reaction to a common sulfa based antibiotic. This particular antibiotic is perhaps the most widely prescribed antibiotic in the outpatient setting. Side effects of this type occur very infrequently, but since it is widely prescribed, such rare events happen. In this case no one contests that the reactions are real, even though it is only a vanishing small fraction of people who take this drug who develop this severe and potentially life threatening complication.

There are also drug related events where bad outcomes happen in association with particular medications, and it is hotly contested whether these outcomes are causally related to the medication taken. The way the FDA regulations are applied is that if a novel life threatening event occurs when a patient takes a particular new drug, the FDA is empowered to change the drug labeling. They are within their powers to require inclusion of a block box warning, when the causality can be shown or not. Drugs widely prescribed to sick populations can be virtually guaranteed to get linked to spectacularly bad outcomes and their package inserts will, over time, become littered with all sorts of warnings, whether causally linked or not. Even if large scale studies are completed and call particular links to drug induced outcomes into question, the labels rarely if ever get changed, much to the delight of trial lawyers. Absence of proof is never proof of absence and even the perception of causality can be leveraged into big bucks. In the world of health you do not need proof of harm to act, only plausible perception.
We need also to touch upon the effect of the coarsening of the media and its possible effects on people undertaking acts of violence. This question has been raised with every form of media at some point in the past; books, film, music, TV. Most recently the age old debate is raging around the effects of computer games. I am of the age where my children were among the first generation of those who had computer games from the earliest points of their lives. I saw the gradual evolution of these games from crude graphics (in space invaders) to the evolution of very graphic, very real appearing creatures and every day life circumstances.

We had our share of children and ultimately teenagers in our basement shooting things up on the big screen. When it started it was the Mario brothers and an odd menagerie of villains. This evolved into more people-like characters in war like games. At that time the on screen entities were more creatures than people and it did not occur to me that our children could be getting conditioned to commit violent acts against actual people. It was a gradual evolution. From what I have previewed online, some games are remarkably life like and the violence committed on screen is gratuitous and aimed at the innocent and defenseless.

It only makes sense that viewing violent acts chronically is not healthy. It has long been appreciated that living in a violent household teaches children to use violence to achieve their ends. Why those immersed in a virtual violent world should be immune to these influences is hard to fathom. It has been suggested that violent videos might facilitate a form of release and prevent violence. Based upon that logic, we should encourage violence in the home so as to prevent violence outside the household. I don't think it works that way.
Much in the same way we in medicine observe low frequency events which appear to be causally linked to particular medication exposures, our present experiences with violent mass killers appears to associated preferentially (if not exclusively) with young men who have played lots of violent first person shooter games. Yes, many young men play violent first person shooter games and do not go on to be mass murderers. However, millions of people take Bactrim and Tegretol and never have any problems with these drugs. Should that lead us to believe that the innocuous experience of the many should convince us of no linkage to the catastrophic effects on the rare few? Just because one million people can take these drugs with no harm does not negate the fact that one in a million will be devastated.
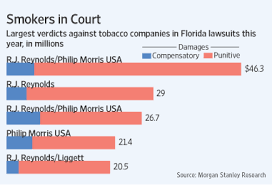
I am sure that the media companies who produce such games will rally around the first amendment for protection. Just because they may be legally protected from state restrictions does not mean their product does not cause harm. This brings to mind the denial of the tobacco companies, who maintained the safety of their product despite similar correlational evidence linking it to harm. The actual epidemiology evidence linking smoking to health harms followed only initial anecdotal observations of harm. The similarities are there. Both exposures required chronic and excessive exposure over long periods of time. Not all who were exposed were harmed.
I have no desire to parley the possibility of negative influence of first person shooter games to argue for some sort of state regulation. That basically never works and the unintended consequences of using blunt legal tools to restrict access targeting only a tiny minority far outweighs whatever good that comes of such attempts. That said, we cannot stay in denial that our brains are heavily influenced by repeated exposure to violent images and virtual world violence. It may not have profound effects on most people who are exposed but, in my opinion, there is enough empiric evidence from early formal studies and recent events to encourage caution, particularly in parents (http://futureofchildren.org/futureofchildren/publications/docs/12_02_05.pdf). Ultimately social stigma and informal restriction from the mainstream may be more effective for control than any legal mandates. However, there must be recognition that these games are not healthy and that is is not unreasonable to have the concern that intense and long term exposure to virtual violence may influence select people to do terrible acts. This is not a popular message from the usual media outlets since there is a huge conflict of interest. They are loathe to draw any attention to this possibility.
I also will not be surprised if the violent video game industry moves into the cross hairs of the trial attorneys. The data showing violent first person shooter games change behavior is only now developing. I would not be at all surprised if grieving families who have lost loved ones to violence facilitated by immersion in violent media. While the mass shootings gain the spotlight, I suspect that there is a much larger pool of violent acts where violent games play a role. We do not have the epidemiological tools to appreciate them yet. It is just a matter of time before the trial bar lays claim to their ill gained earnings. They will be held to a similar standard as those within the health care field.

