
From Art Diamond's blog
http://www.artdiamondblog.com/archives/2010/01/_michael_hicks.html
Universal law of screening. Dial up the sensitivity and you lose specificity. On the flip side, go for specificity and you lose sensitivity. It operates this way when screening for terrorists and cancer.
Sunday, January 31, 2010
The limits of planning
Plans are nothing; planning is everything.
Dwight D. Eisenhower
One of the consistent observations reported back from Haiti has been that volunteers have been struck by the lack of basic infrastructure which has made their work nearly impossible. While tragic and terrible, this should come as no surprise. When we make plans, particularly for rare and terrible events, there are many assumptions which go unnoticed, that is until execution is needed. We assume that certain basic resources will be in place. For example, no one considers whether there will be air to breathe. That is a given unless the rescue mission is to the moon or perhaps to some lake in central Africa where methane poisoning may be a consideration.
In Haiti, we assumed that despite the destruction there would be a certain basic social and political infrastructure. That assumption was not correct. Haiti's tragic history is to a great degree a consequence of that never developing. Despite the huge humanitarian deployment, that infrastructure cannot be created overnight, particularly within the context of the destruction of the limited physical infrastructure which existed.
"Happiness equals reality minus expectations" - Tom Magliozzi
This is one of my favorite quotes, from the great philosophical sages of the 20th century. It is very timely in terms of how we view the possible responses to the predictably unpredictable tragedies which have always occurred and will always occur in our world. Which one is next? Will it be an earthquake which devastates southern California or Memphis, a Hurricane which hits south Florida, the explosion of the Yellowstone Caldera which may cover the eastern portion of the US under a foot of ash, or the explosion of a suitcase nuclear device in New York or Washington. The possibilities are endless. Can we plan for all of them? In the event of such a catastrophe, how will we actually assess what success is? I could imagine a scenario where planning and execution are outstanding, yet thousands might die and the entire activity deemed a total failure despite saving countless lives.
How best to deal proactively with possible catastrophe? One asset we in the US have which Haiti does not have is the reserve which comes as a consequence of being wealthy. With wealth comes some degree of wiggle room which is simply not available when you are living hand to mouth. The benefits of this permeate into virtually all elements that will be touched by physical catastrophes. Greater wealth allows for more stringent building codes and the tax base to support first responder networks.
http://haitirewired.wired.com/profiles/blogs/engineer-this-was-not-an?utm_source=feedburner&utm_medium=feed&utm_campaign=Feed:+wired/index+(Wired:+Index+3+(Top+Stories+2))&utm_content=Google+Reader
It allows for those who have some reserve to use saved assets to use them to hire private support systems. Wealthy companies such as Walmart were instrumental in using their supply chains to deliver aid after Katrina. Wealthy people shared their private resources to aid those affected.
Perhaps the best plan to deal with catastrophe is to create expectations that the best way to survive a catastrophe is to always plan to have substantial private assets which are deployable or have been previously invested to blunt the impact. Governments simply cannot replace the private planning. Furthermore, any policy which encourages the formation of individual wealth may be the best insurance policy for surviving catastrophe that we will ever have.
"Happiness equals reality minus expectations" - Tom Magliozzi
This is one of my favorite quotes, from the great philosophical sages of the 20th century. It is very timely in terms of how we view the possible responses to the predictably unpredictable tragedies which have always occurred and will always occur in our world. Which one is next? Will it be an earthquake which devastates southern California or Memphis, a Hurricane which hits south Florida, the explosion of the Yellowstone Caldera which may cover the eastern portion of the US under a foot of ash, or the explosion of a suitcase nuclear device in New York or Washington. The possibilities are endless. Can we plan for all of them? In the event of such a catastrophe, how will we actually assess what success is? I could imagine a scenario where planning and execution are outstanding, yet thousands might die and the entire activity deemed a total failure despite saving countless lives.
In our 21st century world, we make huge investments in both physical and social infrastructure to make our lives better, primarily to protect us from physical wants and discomfort. In a primitive world physical catastrophe does not destroy much. Those who survive may be able to rapidly get back to their baseline status, as poor as it might be. In our world marked by complex physical infrastructure which is required to support our complex social interdependencies, physical catastrophe results in much more loss than the individual lives.
We have a certain set of expectations as to what is required for us to "survive" and these expectations are quite different from what they were 50 or 100 years ago. When Herbert Hoover spearheaded the efforts to save those devastated by the great 1927 floods of the Mississippi River, those who his efforts saved had few if any expectations. Furthermore, when the waters receded there was precious little to rebuild in comparison to what would be required now. The physical infrastructure is just much more complex now.
This makes planning for disasters more and more difficult. When I was involved with a medical center IT planning project one aspect we discussed is how to plan for rapid deployment of IT infrastructure to get back online in the event of some sort of catastrophic event. Beyond the data backup, how much of the hardware needed to be redundant and where? If we are to have redundant IT infrastructure, what about other infrastructure such as core services such as pathology, radiology, operative suites, and emergency services. Should we build a completely redundant "mirror" hospital to have just in case? Who would pay for and maintain this? Is this type of insurance really necessary?
I think the lesson is the downside of sophisticated infrastructure which makes our lives better is like any sort of leverage. It can cut both ways. Without such infrastructure, we are destined to suffer every day. With such infrastructure our lives are better but we we become dependent upon it and in the rare event where catastrophe hits, the devastation and the rebuilding process is terribly painful. Furthermore, we should not create expectations that we can plan for total effective interventions for all such eventualities at a local, state, or national levels.
How best to deal proactively with possible catastrophe? One asset we in the US have which Haiti does not have is the reserve which comes as a consequence of being wealthy. With wealth comes some degree of wiggle room which is simply not available when you are living hand to mouth. The benefits of this permeate into virtually all elements that will be touched by physical catastrophes. Greater wealth allows for more stringent building codes and the tax base to support first responder networks.
http://haitirewired.wired.com/profiles/blogs/engineer-this-was-not-an?utm_source=feedburner&utm_medium=feed&utm_campaign=Feed:+wired/index+(Wired:+Index+3+(Top+Stories+2))&utm_content=Google+Reader
It allows for those who have some reserve to use saved assets to use them to hire private support systems. Wealthy companies such as Walmart were instrumental in using their supply chains to deliver aid after Katrina. Wealthy people shared their private resources to aid those affected.
Perhaps the best plan to deal with catastrophe is to create expectations that the best way to survive a catastrophe is to always plan to have substantial private assets which are deployable or have been previously invested to blunt the impact. Governments simply cannot replace the private planning. Furthermore, any policy which encourages the formation of individual wealth may be the best insurance policy for surviving catastrophe that we will ever have.
Haiti aid- Ramblings regarding planning, healthcare pricing, allocation, and distribution
In today's paper, there was a story about the state of Florida saying "uncle" regarding further transfer of injured Haitians to Florida hospitals. Obviously this was met with dismay from the legions of volunteers in Haiti who are committing their time and effort in an heroic effort to save as many lives as possible. However, trauma care in the US is a contracting resource and there is every reason to believe that the Haitian crisis has saturated the Florida system, putting them in a position which could be completely anticipated; that is it was not whether if they had to say no but in fact when they had to put the brakes on how many patients they can care for.
Trauma care in the country is one of the major areas which has been crippled by administrative pricing structures and unwise regulatory incursions. These are well delineated in a 2004 document published by the National Foundation for Trauma Care.
http://www.traumacare.com/download/NFTC_CrisisReport_May04.pdf
The bottom line is that trauma care loses money and that financial losses will lead to continued closing of trauma centers. It is completely unrealistic to believe that any planning efforts related to natural or man made (e.g. terror) catastrophes can be dealt with if the main bottleneck is the capacity to handle injured or sick people.
Trauma care loses money because of a variety of issues including the impact of uninsured patients. However an additional factor is the administrative pricing structure of payments. In particular, it the inappropriately low reimbursement from public insurers (Medicare and Medicaid) which is sinking trauma centers. Even if all the uninsured were covered by public insurance, trauma care would still be a money loser.
In order to avoid stinting of an already scarce resource, the Federal government created EMTALA. Unfortunately the unintended consequence of EMTALA is to further disincentivize hospitals from providing trauma care. When services lose lots of money, the business case for discontinuing such services becomes overwhelmingly compelling. Business entities which sustain losses for extended periods have one thing in common. They cease to exist.
I often hear arguments that we live in such a wealth country that there should be no poverty or want. This mindset focuses on the allocation aspect as a determinant of wealth or poverty. Haiti should stand as a stark example that allocation is only a small piece to the "why are people/places rich or poor" question. The major piece is creation of the resources which determine wealth. We are no in a position to offer unlimited trauma hospital resources to the injured in Haiti because those resources have not been created and even if they had been created in the past, we have created economic incentives to dismantle them.
The lesson is you cannot allocate what has not been created and that which is valued at less than the costs of production does not get created. At the heart of this problem is the information transmitted by an administrative pricing structure which predictably undervalues some things and has no reliable mechanism for self correction. You cannot centrally predict which specific things will be undervalued and the shortages that will result, only that many things will be priced wrong. You cannot legislate critical resources into existence although it appears that you can readily legislate them out of existence. It is inherently easier to destroy things than to build them.
Trauma care in the country is one of the major areas which has been crippled by administrative pricing structures and unwise regulatory incursions. These are well delineated in a 2004 document published by the National Foundation for Trauma Care.
http://www.traumacare.com/download/NFTC_CrisisReport_May04.pdf
The bottom line is that trauma care loses money and that financial losses will lead to continued closing of trauma centers. It is completely unrealistic to believe that any planning efforts related to natural or man made (e.g. terror) catastrophes can be dealt with if the main bottleneck is the capacity to handle injured or sick people.
Trauma care loses money because of a variety of issues including the impact of uninsured patients. However an additional factor is the administrative pricing structure of payments. In particular, it the inappropriately low reimbursement from public insurers (Medicare and Medicaid) which is sinking trauma centers. Even if all the uninsured were covered by public insurance, trauma care would still be a money loser.
In order to avoid stinting of an already scarce resource, the Federal government created EMTALA. Unfortunately the unintended consequence of EMTALA is to further disincentivize hospitals from providing trauma care. When services lose lots of money, the business case for discontinuing such services becomes overwhelmingly compelling. Business entities which sustain losses for extended periods have one thing in common. They cease to exist.
I often hear arguments that we live in such a wealth country that there should be no poverty or want. This mindset focuses on the allocation aspect as a determinant of wealth or poverty. Haiti should stand as a stark example that allocation is only a small piece to the "why are people/places rich or poor" question. The major piece is creation of the resources which determine wealth. We are no in a position to offer unlimited trauma hospital resources to the injured in Haiti because those resources have not been created and even if they had been created in the past, we have created economic incentives to dismantle them.
The lesson is you cannot allocate what has not been created and that which is valued at less than the costs of production does not get created. At the heart of this problem is the information transmitted by an administrative pricing structure which predictably undervalues some things and has no reliable mechanism for self correction. You cannot centrally predict which specific things will be undervalued and the shortages that will result, only that many things will be priced wrong. You cannot legislate critical resources into existence although it appears that you can readily legislate them out of existence. It is inherently easier to destroy things than to build them.
Saturday, January 30, 2010
The trap of small numbers
Toyota has a problem. While Toyota is generally referred to in medical circles in reference to its lean processes and potential application to delivery of health care, there are parallels in other areas as well. Toyota has announced it will stop production of a large segment of their product line in order to address problems with uncontrolled acceleration. In 2008, there were 52 complaints to Consumer Reports relating to this problem. This is in the background of the sale of almost nine million cars, about two thirds of these in the US. To make the math simple, let us assume that Toyota sold about five million cars in the US. That means this issue appears to have been reported in approximately 0.0001% percent of sales.
When you start to look at low frequency events like this and try to make sense out of causality, it is problematic. It is hard to to separate random events from linked events, signals vs. noise. This would not be a problem except that low frequency and often spectacularly bad outcomes tend to drive some sort of response and responses mean investment of time, effort, and resources. Again, all of this would be fine if that investment yielded some some of result where the inputs were exceeded by the outputs.
I know I run the risk of critics who might claim that when lives are at stake, money is no object. That is nonsense. If that were the case the only thing we should ever invest in is to save lives. We utilize resources to further other ends, resources which could be allocated to save someone's life. We need to recognize that there is more at stake in living our lives than life and death (see previous blog).
Reaction to low frequency events is not limited to the automobile industry. These types of responses are common to virtually every realm of human activity. The TSA is a huge investment in response to low frequency events. In this case there is an unambiguous link between terrorists blowing up or crashing planes and human lives lost. Whether there is a link between the huge sums invested in TSA and the frequency of lives lost is an open question.
Medicine is absolutely riddled with dogmatic recommendations based upon responses to low frequency events. Read any drug monogram and you will see exhaustive lists of reported symptoms and outcomes which occur in vanishingly small percentages of patients which may or may not occur with any greater frequency than in any control group. Rare disease associations with mundane symptoms or non-specific clinical findings are highlighted in such a way that we respond as if the outlier events were the norm. We develop surveillance programs for drug and disease monitoring which are driven by risk avoidance, even if the risk is vanishingly small or non-existent and the components of the surveillance program may create even more risks than they alleviate.
There is a tendency to blame the fear of lawsuits as the driver of this culture. While this may be true to some degree, I have been in medicine long enough to see that perhaps we have gotten our sequence backwards. Even before malpractice concerns were front burner we adopted a culture within medicine that no amount of effort or resources expended were too great. An inexpensive intervention or approach which yielded a good outcome in 98% of the time would be ditched for something that costs 10x more for a good outcome 98.5% of the time. At least part of the driver might have also been that more expensive approaches yielded higher margins as well. Everyone came out ahead...sort of. As the medical profession adopted expensive approaches to deal with vanishing small improvements in patient outcomes and these approaches became standard of care, the legal profession was all to happy to use this as a business opportunity.
While my experience with being an expert witness is limited, what is common to the dozen or so cases I have participated in is all of them deal with low frequency events. The gut response to such rare and catastrophic occurrences is to look for changes in how one deals with mundane clinical encounters which may result in spectacularly bad outcomes. What to do when a patient presents with a headache, or fever and a rash, or a productive cough? There are unquestionable anecdotes where each of these scenarios is followed by the tragic death of those affected, despite what appears to be appropriate conservative management.
Why not maintain a full court press all of the time and do as much for anyone who might be at risk for a bad outcome? The problem is we live in a work were resources are not infinite and use of resources for a non-productive end means that they cannot be used for something with a more productive outcome. It seems obvious from 20,000 feet but is never obvious when functioning one patient at a time.
So, what to do? Much of the decision as to what to do will boil down to needing data. When we are tempted to act to forestall some bad outcome which occurs very rarely, we need to identify just how likely the bad event might be. I am not talking about defining possibilities down to precise numbers but trying to begin define them in terms of orders of magnitude. Do these things happen 50% , 0.5%, or .0005% of the time. Also, there is a tendency to track surrogate endpoints because measuring what is really important is so difficult or the events which we are trying to avoid are so rare. If the endpoints we are trying to avoid are so rare that we have a hard time measuring them, perhaps that says something about where they should be viewed as priorities.
Ultimately is comes down to culture change. We must change the culture within medicine where physicians begin to understand numbers, recognize their limitations, and convey these concepts to patients. We must change the expectation of patients where they realize there are always risks and that all interventions carry potential unintended consequences. It is a tall order.
When you start to look at low frequency events like this and try to make sense out of causality, it is problematic. It is hard to to separate random events from linked events, signals vs. noise. This would not be a problem except that low frequency and often spectacularly bad outcomes tend to drive some sort of response and responses mean investment of time, effort, and resources. Again, all of this would be fine if that investment yielded some some of result where the inputs were exceeded by the outputs.
I know I run the risk of critics who might claim that when lives are at stake, money is no object. That is nonsense. If that were the case the only thing we should ever invest in is to save lives. We utilize resources to further other ends, resources which could be allocated to save someone's life. We need to recognize that there is more at stake in living our lives than life and death (see previous blog).
Reaction to low frequency events is not limited to the automobile industry. These types of responses are common to virtually every realm of human activity. The TSA is a huge investment in response to low frequency events. In this case there is an unambiguous link between terrorists blowing up or crashing planes and human lives lost. Whether there is a link between the huge sums invested in TSA and the frequency of lives lost is an open question.
Medicine is absolutely riddled with dogmatic recommendations based upon responses to low frequency events. Read any drug monogram and you will see exhaustive lists of reported symptoms and outcomes which occur in vanishingly small percentages of patients which may or may not occur with any greater frequency than in any control group. Rare disease associations with mundane symptoms or non-specific clinical findings are highlighted in such a way that we respond as if the outlier events were the norm. We develop surveillance programs for drug and disease monitoring which are driven by risk avoidance, even if the risk is vanishingly small or non-existent and the components of the surveillance program may create even more risks than they alleviate.
There is a tendency to blame the fear of lawsuits as the driver of this culture. While this may be true to some degree, I have been in medicine long enough to see that perhaps we have gotten our sequence backwards. Even before malpractice concerns were front burner we adopted a culture within medicine that no amount of effort or resources expended were too great. An inexpensive intervention or approach which yielded a good outcome in 98% of the time would be ditched for something that costs 10x more for a good outcome 98.5% of the time. At least part of the driver might have also been that more expensive approaches yielded higher margins as well. Everyone came out ahead...sort of. As the medical profession adopted expensive approaches to deal with vanishing small improvements in patient outcomes and these approaches became standard of care, the legal profession was all to happy to use this as a business opportunity.
While my experience with being an expert witness is limited, what is common to the dozen or so cases I have participated in is all of them deal with low frequency events. The gut response to such rare and catastrophic occurrences is to look for changes in how one deals with mundane clinical encounters which may result in spectacularly bad outcomes. What to do when a patient presents with a headache, or fever and a rash, or a productive cough? There are unquestionable anecdotes where each of these scenarios is followed by the tragic death of those affected, despite what appears to be appropriate conservative management.
Why not maintain a full court press all of the time and do as much for anyone who might be at risk for a bad outcome? The problem is we live in a work were resources are not infinite and use of resources for a non-productive end means that they cannot be used for something with a more productive outcome. It seems obvious from 20,000 feet but is never obvious when functioning one patient at a time.
So, what to do? Much of the decision as to what to do will boil down to needing data. When we are tempted to act to forestall some bad outcome which occurs very rarely, we need to identify just how likely the bad event might be. I am not talking about defining possibilities down to precise numbers but trying to begin define them in terms of orders of magnitude. Do these things happen 50% , 0.5%, or .0005% of the time. Also, there is a tendency to track surrogate endpoints because measuring what is really important is so difficult or the events which we are trying to avoid are so rare. If the endpoints we are trying to avoid are so rare that we have a hard time measuring them, perhaps that says something about where they should be viewed as priorities.
Ultimately is comes down to culture change. We must change the culture within medicine where physicians begin to understand numbers, recognize their limitations, and convey these concepts to patients. We must change the expectation of patients where they realize there are always risks and that all interventions carry potential unintended consequences. It is a tall order.
Wednesday, January 27, 2010
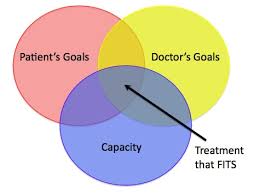
Whose goals are we focused on?
I hold a leadership position in an academic medical center and, although my practice is almost exclusively outpatient based, I am heavily involved in various activities which focus on inpatient quality metrics. There is a stark contrast between the stakes involved with hospitalized patients and the stakes involved with those followed in the ambulatory setting. Patients in the hospital are generally in settings with a high risk of death, either because of underlying disease, planned interventions, or both. Not only are the stakes high in terms of ultimate outcomes, but they tend to be high financial stakes as well. Deservedly, much emphasis is placed on this environment.
 However, most physician-patient encounters occur outside of this high stakes world. As important as the life and death metrics might be, we cannot ignore the day to day goals and struggles of patients who are affected by illness. If our only focus are metrics which examine whether interventions affect whether patients live or die, we will not improve the lives of those destined to live with disease. Most disease does not kill patients but constitutes disease because it causes suffering, and functional impairment.
However, most physician-patient encounters occur outside of this high stakes world. As important as the life and death metrics might be, we cannot ignore the day to day goals and struggles of patients who are affected by illness. If our only focus are metrics which examine whether interventions affect whether patients live or die, we will not improve the lives of those destined to live with disease. Most disease does not kill patients but constitutes disease because it causes suffering, and functional impairment.
To a great extent impact into daily quality of life falls within the realm of how medicine impacts people in the mundane world of outpatients. This is where people spend the overwhelming majority of their lives. One of the great limitations we face is a huge information deficit in this realm. Even the most closely observed outpatient may interface with their physician or extender a few minutes every week and more likely every few months. Our end points as providers are measured after weeks, months, or years and even our most stellar successes are punctuated by constant suffering while we wait for our end points.
Virtually none of my training has made me particularly aware of the challenges my patients face in dealing with their chronic diseases, every day. In addition there are few financial rewards (actually no financial rewards) for devoting time to expanding our awareness of such issues. Even if we become aware, we have little additional insight relating to novel coping mechanisms which allow patients to deal with disease morbidity, It is not part of our training, nor is it a research focus. We are simply not particularly aware and there are few initiatives to look for the gaps.
Beyond saving lives, what is our mission? It is my opinion that our goals as physicians are seriously misaligned with the goals of our patients. We are focused on what we believe they need and are dismissive of the possibility that we should be focused on what patients want. In order to accomplish this end we need to start by determining how disease impacts patients and their families in their daily lives. Perhaps the impact may not rise to the level of life and death but it is terribly important nonetheless.
We need to become serious about asking these questions, developing tools to assess impact, and then look at these as legitimate endpoints for looking at the efficacy of interventions. We need to realize that the so called hard objective endpoints may simply be surrogate endpoints which may or may not track with what patients value more.
To a great extent impact into daily quality of life falls within the realm of how medicine impacts people in the mundane world of outpatients. This is where people spend the overwhelming majority of their lives. One of the great limitations we face is a huge information deficit in this realm. Even the most closely observed outpatient may interface with their physician or extender a few minutes every week and more likely every few months. Our end points as providers are measured after weeks, months, or years and even our most stellar successes are punctuated by constant suffering while we wait for our end points.
Virtually none of my training has made me particularly aware of the challenges my patients face in dealing with their chronic diseases, every day. In addition there are few financial rewards (actually no financial rewards) for devoting time to expanding our awareness of such issues. Even if we become aware, we have little additional insight relating to novel coping mechanisms which allow patients to deal with disease morbidity, It is not part of our training, nor is it a research focus. We are simply not particularly aware and there are few initiatives to look for the gaps.
Beyond saving lives, what is our mission? It is my opinion that our goals as physicians are seriously misaligned with the goals of our patients. We are focused on what we believe they need and are dismissive of the possibility that we should be focused on what patients want. In order to accomplish this end we need to start by determining how disease impacts patients and their families in their daily lives. Perhaps the impact may not rise to the level of life and death but it is terribly important nonetheless.
We need to become serious about asking these questions, developing tools to assess impact, and then look at these as legitimate endpoints for looking at the efficacy of interventions. We need to realize that the so called hard objective endpoints may simply be surrogate endpoints which may or may not track with what patients value more.
Sunday, January 24, 2010
Am I hearing this correctly?
The Supreme court issued a split ruling on legislative limits placed on corporate support of political activities. The ruling lifted restrictions on corporate funding based upon an interpretation of the constitution which basically finds no justification for the government to place limits political speech, either by individuals of by individuals banded together voluntarily in the form of corporations. The NY Times issued a scathing editorial attacking the court decision.
http://www.nytimes.com/2010/01/22/opinion/22fri1.html
The first amendment is very brief and simply states:
The language is starkly simple. I see no exceptions guaranteeing freedom of speech only to single individuals here. Which brings me to the second line in the NYT piece calling upon Congress to act. Did they not read the Constitution where it says " Congress shall make no law."? Why should they think that the way to address the first amendment, which prohibits Congress from acting to abridge free speech, is to implore Congress to act to abridge free speech?
It appears that their background on US History is somewhat lacking. Remember, the Bill of Rights was added because there was great concern that the citizenry required greater protections from incursions of the state, not as a brake on private activity of citizens, either singly or in the form of volunteer associations.
The Times protestations are somewhat disingenuous since they are a corporation. However, the law as previously conceived created exemptions for media of certain types. The exemption is based upon an obsolete conception of the press and corporations. This creates all sorts of ambiguities which can serve as an impediment to free speech. This is well summarized in the DeMoines Register:
It seems pretty straight forward to me. On the side of human freedom is the narrow majority of the court who interpret the plain language of the first amendment as it sounds. The opposition wants to empower the state to squelch speech of individuals banded together in voluntary associations, with certain ill defined and politically exploitable exceptions.
http://www.nytimes.com/2010/01/22/opinion/22fri1.html
The Court’s Blow to Democracy
With a single, disastrous 5-to-4 ruling, the Supreme Court has thrust politics back to the robber-baron era of the 19th century. Disingenuously waving the flag of the First Amendment, the court’s conservative majority has paved the way for corporations to use their vast treasuries to overwhelm elections and intimidate elected officials into doing their bidding.
Congress must act immediately to limit the damage of this radical decision, which strikes at the heart of democracy.....
The first amendment is very brief and simply states:
Congress shall make no law respecting an establishment of religion, or prohibiting the free exercise thereof; or abridging the freedom of speech, or of the press; or the right of the people peaceably to assemble, and to petition the Government for a redress of grievances.
The language is starkly simple. I see no exceptions guaranteeing freedom of speech only to single individuals here. Which brings me to the second line in the NYT piece calling upon Congress to act. Did they not read the Constitution where it says " Congress shall make no law."? Why should they think that the way to address the first amendment, which prohibits Congress from acting to abridge free speech, is to implore Congress to act to abridge free speech?
It appears that their background on US History is somewhat lacking. Remember, the Bill of Rights was added because there was great concern that the citizenry required greater protections from incursions of the state, not as a brake on private activity of citizens, either singly or in the form of volunteer associations.
The Times protestations are somewhat disingenuous since they are a corporation. However, the law as previously conceived created exemptions for media of certain types. The exemption is based upon an obsolete conception of the press and corporations. This creates all sorts of ambiguities which can serve as an impediment to free speech. This is well summarized in the DeMoines Register:
http://blogs.desmoinesregister.com/dmr/index.php/2010/01/23/speech/
The Opinion makes an excellent point about corporations involved in the news business. Freedom of the press was a clear intent of the Framers. In order to restrict corporate political activity, exemptions have to be made for those corporations involved in the media. This gives one company rights another does not have and that is unfair. Laws that permit a company that owns a newspaper to promote a candidate or issue whenever and however they like, but restrict a non-media company from doing the same are inherently biased.
The Opinion also speaks to the decline of print and broadcast media and the rise of the Internet and new forms of communication. The line between the media and others who wish to comment on political and social issues has become blurred.
It seems pretty straight forward to me. On the side of human freedom is the narrow majority of the court who interpret the plain language of the first amendment as it sounds. The opposition wants to empower the state to squelch speech of individuals banded together in voluntary associations, with certain ill defined and politically exploitable exceptions.
Saturday, January 23, 2010
Is there a universal lesson here?
I was doing my perusal of Arts and Letters daily and I came upon an article in the Wilson Quarterly. It is funny, I used to be an avid reader of this, saving every issue for more than 20 years until my subscription lapsed. I am not sure why that happened. I must have gotten distracted with something else.
While the original link from A&L daily was to one article, I got distracted and found another centered around a "radical" traffic engineer by the name of Hans Monderman.
http://www.wilsoncenter.org/index.cfm?fuseaction=wq.essay&essay_id=462572
I can see all sorts of parallels and ironies. Attempts to domesticate life and create safety are always complicated by creating moral hazards. When you insulate people from dangers, you also run the risk of altering their behavior in such a way that creates new risks. Obviously it makes sense to at least try to identify risky circumstances and at least go after the low hanging fruit. However, an important safety mechanism is our own vigilance which is tightly linked to worry and anxiety, arguably emotions which we would just as well avoid. How do you create safe environments which do not lull us into false senses of security?
These observations have implications which touch virtually all elements of human life. When the economy is going well and the stock market soaring, can this only happen when there is sufficient confidence which may very well be compatible with the lack of worry? Creation of financial backstops in the name of safety may foster behaviors which create greater risks.
Has the increasing the power of our medical tools created an illusion of safety which fosters behaviors which create more hazards? Do we take physical risks when we are young based upon the assumption that injuries can be repaired. Do we imbibe in dietary indiscretions based upon the assumption that the risks created can be undone using pharmacological interventions or stents?
In contrast, flying is in an environment which is both safer and associated with greater fear. Is that a good thing? How (and should) we create environments which are both safer and associated with the impression of not being safer? Will we put up with this? Is that what we should want?
While the original link from A&L daily was to one article, I got distracted and found another centered around a "radical" traffic engineer by the name of Hans Monderman.
http://www.wilsoncenter.org/index.cfm?fuseaction=wq.essay&essay_id=462572
And Monderman certainly changed the landscape in the provincial city of Drachten, with the project that, in 2001, made his name. At the town center, in a crowded four- way intersection called the Lawei plein, Monderman removed not only the traffic lights but virtually every other traffic control. Instead of a space cluttered with poles, lights, “traffic islands,” and restrictive arrows, Monderman installed a radical kind of roundabout (a “squareabout,” in his words, because it really seemed more a town square than a traditional roundabout), marked only by a raised circle of grass in the middle, several fountains, and some very discreet indicators of the direction of traffic, which were required by law.
As I watched the intricate social ballet that occurred as cars and bikes slowed to enter the circle (pedestrians were meant to cross at crosswalks placed a bit before the intersection), Monderman performed a favorite trick. He walked, backward and with eyes closed, into the Laweiplein. The traffic made its way around him. No one honked, he wasn’t struck. Instead of a binary, mechanistic process—stop, go—the movement of traffic and pedestrians in the circle felt human and organic.
A year after the change, the results of this “extreme makeover” were striking: Not only had congestion decreased in the intersection— buses spent less time waiting to get through, for example— but there were half as many accidents, even though total car traffic was up by a third. Students from a local engineering college who studied the intersection reported that both drivers and, unusually, cyclists were using signals— of the electronic or hand variety— more often. They also found, in surveys, that residents, despite the measurable increase in safety, perceived the place to be more dangerous. This was music to Monderman’s ears. If they had not felt less secure, he said, he “would have changed it immediately.”
I can see all sorts of parallels and ironies. Attempts to domesticate life and create safety are always complicated by creating moral hazards. When you insulate people from dangers, you also run the risk of altering their behavior in such a way that creates new risks. Obviously it makes sense to at least try to identify risky circumstances and at least go after the low hanging fruit. However, an important safety mechanism is our own vigilance which is tightly linked to worry and anxiety, arguably emotions which we would just as well avoid. How do you create safe environments which do not lull us into false senses of security?
These observations have implications which touch virtually all elements of human life. When the economy is going well and the stock market soaring, can this only happen when there is sufficient confidence which may very well be compatible with the lack of worry? Creation of financial backstops in the name of safety may foster behaviors which create greater risks.
Has the increasing the power of our medical tools created an illusion of safety which fosters behaviors which create more hazards? Do we take physical risks when we are young based upon the assumption that injuries can be repaired. Do we imbibe in dietary indiscretions based upon the assumption that the risks created can be undone using pharmacological interventions or stents?
In contrast, flying is in an environment which is both safer and associated with greater fear. Is that a good thing? How (and should) we create environments which are both safer and associated with the impression of not being safer? Will we put up with this? Is that what we should want?
Friday, January 22, 2010
The health care end game
Now that the Massachusetts election is behind us and the health care express has been derailed, everyone is asking "Now what is the next step?" Ironies abound, not the least of which is the very senate seat, which was occupied for more than 40 years by one of the major driver of health care reform, is the very seat which will tip the balance toward sending this initiative to the dustbin of history. You could not script this any better to capture the almost tragedy like quality. The end of the Kennedy era in politics going out with a whimper as opposed to a bang.
What will be the next step? If you are under the impression that the failure of legislative reform means no change in health care payments, you will be sadly mistaken. We are quickly approaching a rock and hard place scenario which, if anything, will be aggravated by the failure of passage of the so called reform bill. That legislation, in either the House or Senate format, would have pumped in huge additional dollars to keep the health care bubble inflated. It is not clear at this point in time whether the SGR fix will be extended beyond the end of February. Who will champion this? Who should champion this? What will happen if Medicare payments are cut by over 20%?
The blunt instrument a 20% Medicare cut will be will result in taking down those who operate at the lower margins who cannot further cut their costs. It will yet again reward those who best the gamed the system by being the most greedy in the past and punish those whose emphasis has been lower cost care. As grim as this sounds, this threat can also represent opportunity. Once Medicare becomes sufficiently unattractive, we may observe a critical mass of providers to attempt to develop a new, Medicare independent business models. Based upon Christensen's disruptive model, I would envision it starting in the low margin arena. Perhaps blood pressure management clinics which use generic medications or protocol driven depression treatment clinics. Most will fail miserably but some will flourish.
I could also envision non-physicians take on roles as coordinators of care. Whether such work would require licensing or specific training if their job were to simply give advice for a nominal fee is possible. It represents work which at this point has no margins and it would be activity which physicians would likely abandon in a heartbeat. Whether the business model would be through fee for service or a subscription model, or whether many of the queries could be addressed via defined protocols or artificial intelligence is an open possibility.
I find when I try to predict the future I am generally wrong on the specifics by right on the concepts. I am certain that when the bubble bursts, innovative lower cost options will grow in the wreckage.
What will be the next step? If you are under the impression that the failure of legislative reform means no change in health care payments, you will be sadly mistaken. We are quickly approaching a rock and hard place scenario which, if anything, will be aggravated by the failure of passage of the so called reform bill. That legislation, in either the House or Senate format, would have pumped in huge additional dollars to keep the health care bubble inflated. It is not clear at this point in time whether the SGR fix will be extended beyond the end of February. Who will champion this? Who should champion this? What will happen if Medicare payments are cut by over 20%?
The blunt instrument a 20% Medicare cut will be will result in taking down those who operate at the lower margins who cannot further cut their costs. It will yet again reward those who best the gamed the system by being the most greedy in the past and punish those whose emphasis has been lower cost care. As grim as this sounds, this threat can also represent opportunity. Once Medicare becomes sufficiently unattractive, we may observe a critical mass of providers to attempt to develop a new, Medicare independent business models. Based upon Christensen's disruptive model, I would envision it starting in the low margin arena. Perhaps blood pressure management clinics which use generic medications or protocol driven depression treatment clinics. Most will fail miserably but some will flourish.
I could also envision non-physicians take on roles as coordinators of care. Whether such work would require licensing or specific training if their job were to simply give advice for a nominal fee is possible. It represents work which at this point has no margins and it would be activity which physicians would likely abandon in a heartbeat. Whether the business model would be through fee for service or a subscription model, or whether many of the queries could be addressed via defined protocols or artificial intelligence is an open possibility.
I find when I try to predict the future I am generally wrong on the specifics by right on the concepts. I am certain that when the bubble bursts, innovative lower cost options will grow in the wreckage.
Tuesday, January 19, 2010
If air travel was like health care video
Yes.. a bit over the top but a good wake up call. Remember, we are in a service industry.
http://jeffreygoldberg.theatlantic.com/archives/2010/01/if_air_travel_worked_like_heal.php
http://jeffreygoldberg.theatlantic.com/archives/2010/01/if_air_travel_worked_like_heal.php
Saturday, January 16, 2010
Another example of a blind spot
After perusing my blog feeds, I came upon Greg Mankiw's blog and a two hour symposium on health care reform at Harvard. It is well worth reading.
http://hms.harvard.edu/public/health_reform/
I particularly enjoyed David Cutler's presentation highlighting the lack of increased productivity in health care, despite huge increases in spending. He highlighted the perverse effect of the payment system on this, stating what everyone has come to realize; the payment system as presently constructed rewards those simply for doing more things. He also notes that the present system has huge administrative burdens. This is not surprising since the return on investment is much greater from investing in billing clerks than RNs. His presentation can be found at:
http://hms.harvard.edu/public/health_reform/img/cutler.pdf
I have a hard time with his firm conclusions that the demand side is not where to operate. He does cite a few studies where patients, when faced with higher out of pocket expenses, elect to cut back on care in some form or another. This is stated to be unquestionably an undesirable effect but these studies do not actually demonstrate worse outcomes. They are short term effects which may in fact create improved outcomes overall but applying price pressures and perhaps creating more affordable health care in the longer term.
My major beef is with his conclusions regarding how health care reform will impact the problems at hand. I completely agree that the major issues are information, incentives, and people. The present payment system creates all the wrong incentives. However, Cutler fails to recognize a key element of the perverse incentives is embedded in the faulty information created by the administrative pricing structure. The proposed reforms simply replace one administrative pricing structure with another. I don't care that he and his colleagues are smart Harvard guys. They are no more capable of creating a workable administrative pricing structure than any of the other very smart people who have failed throughout history. Claims to the contrary amounts to hubris of the worst kind.
Prices are nothing but information which, within market based economies, serve as the critical information required to effectively coordinate human activity. He recognizes that access to information is key to improve productivity and efficiently allocate resources in essentially any industry. Despite frequent claims that health care is different and cannot be allocated primarily via market mechanisms, the recognition that information is key to effectively reform our system is an implicit recognition that we have little choice but use market based pricing mechanisms. What is our choice? How will we figure out the prices otherwise and how can we determine when they are wrong?
http://hms.harvard.edu/public/health_reform/
I particularly enjoyed David Cutler's presentation highlighting the lack of increased productivity in health care, despite huge increases in spending. He highlighted the perverse effect of the payment system on this, stating what everyone has come to realize; the payment system as presently constructed rewards those simply for doing more things. He also notes that the present system has huge administrative burdens. This is not surprising since the return on investment is much greater from investing in billing clerks than RNs. His presentation can be found at:
http://hms.harvard.edu/public/health_reform/img/cutler.pdf
I have a hard time with his firm conclusions that the demand side is not where to operate. He does cite a few studies where patients, when faced with higher out of pocket expenses, elect to cut back on care in some form or another. This is stated to be unquestionably an undesirable effect but these studies do not actually demonstrate worse outcomes. They are short term effects which may in fact create improved outcomes overall but applying price pressures and perhaps creating more affordable health care in the longer term.
My major beef is with his conclusions regarding how health care reform will impact the problems at hand. I completely agree that the major issues are information, incentives, and people. The present payment system creates all the wrong incentives. However, Cutler fails to recognize a key element of the perverse incentives is embedded in the faulty information created by the administrative pricing structure. The proposed reforms simply replace one administrative pricing structure with another. I don't care that he and his colleagues are smart Harvard guys. They are no more capable of creating a workable administrative pricing structure than any of the other very smart people who have failed throughout history. Claims to the contrary amounts to hubris of the worst kind.
Prices are nothing but information which, within market based economies, serve as the critical information required to effectively coordinate human activity. He recognizes that access to information is key to improve productivity and efficiently allocate resources in essentially any industry. Despite frequent claims that health care is different and cannot be allocated primarily via market mechanisms, the recognition that information is key to effectively reform our system is an implicit recognition that we have little choice but use market based pricing mechanisms. What is our choice? How will we figure out the prices otherwise and how can we determine when they are wrong?
Friday, January 15, 2010
At least someone understands the finances
I used to deal with insurance companies in running a small capitated provider network. We complained bitterly when we were not provided with sufficient funds to pay the providers what we thought were appropriate payments for services. As a rule our complaints fell upon deaf ears. We complained yet continued to provide services.
That all changed when we threatened to pull out. At that point negotiations began in earnest. We were previously under the mistaken belief that both we and the insurer were negotiating in good faith. However, in reality negotiations really did not begin until we established credibility by threatening to pull out. We had leverage when it was perceived we were willing to do something which would really put the hurt to those who held the funds.
Today in the WSJ, there was a report on Walgreen's in Washington State threatening to pull out of the Medicaid dispensing business (link below -unfortunately behind the firewall).
http://online.wsj.com/article/SB10001424052748704281204575002651542617666.html?mod=rss_Health#articleTabs%3Darticle
There are certain businesses which have been highly successful in the past decade and the large integrated pharmacy businesses are in that camp. They have deployed sophisticated information and inventory tools which allow them to manage costs and track margins. They have a very focused business model. When an organization like Walgreens threatens to walk away from a huge piece of market share this should serve as a major signal that payments have been set incorrectly. It would be hard to imagine that anyone would want to walk in to fill any void they leave since there would be great fear that unless the payments change it will be an opportunity to lose money.
As the pricing of health care becomes more and more centralized and standardized, there will be more examples where the prices are set too low and providers will walk away. Where lower cost providers can fill the void, that will happen. In some cases it will make little or no difference in terms of patient outcomes. Services of some sort will be rendered, likely of lower quality.
It is difficult to predict specific highly undesirable outcomes. Perhaps large segments of care will simply cease to be available and no one will notice. What is an almost certainty is there will some realms of care which will be tragically under-reimbursed, which will disappear, and have huge impact. The opportunities for this outcome are so great that it is a virtual certainty.
So what will Washington state do if the pharmacy which provides the lion's share of medication dispensing pulls the plug? At least they have some warning. How will other states respond when the the threat is a decentralized one and they wake up one day with no primary care doctors accepting new "insured" patients? Legislatively concocted rights to health care assume that there will always be sufficient resources that can be allocated to fulfill these moral obligations which have been converted to legal ones.
There are always legitimate needs and wants which go unfulfilled because scarcity is a fact of our world. Create punishing mandates to obligate people and businesses to provide services for payments less than the cost and it is the magic formula to make things even scarcer. Unless you can or want to hold a gun to their heads they will walk away. If Walgreens walks away, the state will likely save lots of money be stinting on services. At least everyone (or at least nearly everyone) will have insurance coverage.
That all changed when we threatened to pull out. At that point negotiations began in earnest. We were previously under the mistaken belief that both we and the insurer were negotiating in good faith. However, in reality negotiations really did not begin until we established credibility by threatening to pull out. We had leverage when it was perceived we were willing to do something which would really put the hurt to those who held the funds.
Today in the WSJ, there was a report on Walgreen's in Washington State threatening to pull out of the Medicaid dispensing business (link below -unfortunately behind the firewall).
http://online.wsj.com/article/SB10001424052748704281204575002651542617666.html?mod=rss_Health#articleTabs%3Darticle
Walgreen Co. warned Wednesday night it will withdraw about half of its pharmacies from the state of Washington's Medicaid program Feb. 15 as the program continues to cut back on reimbursements.
The nation's largest drug-store chain made the same vow last year, but a smaller cut in reimbursement rates made Walgreen stand down. A similar standoff occurred last year in Delaware.
The company said Wednesday the most-recent cut in Washington has resulted in Walgreen losing money on the dispensing of 95% of brand-name medications. The reduction, the company said, stems from a Massachusetts court ruling last fall that cut the industry pricing standard "even though pharmacies' acquisition costs haven't changed."
It added, While many private insurance providers have adjusted pharmacy reimbursement rates to limit the impact of the court ruling, Washington's Medicaid program has yet to do so."
Walgreen said it will pull 64 of its pharmacies from the program, representing 75% of the company's total Medicaid business in the state. The company operates 121 pharmacies in Washington.
There are certain businesses which have been highly successful in the past decade and the large integrated pharmacy businesses are in that camp. They have deployed sophisticated information and inventory tools which allow them to manage costs and track margins. They have a very focused business model. When an organization like Walgreens threatens to walk away from a huge piece of market share this should serve as a major signal that payments have been set incorrectly. It would be hard to imagine that anyone would want to walk in to fill any void they leave since there would be great fear that unless the payments change it will be an opportunity to lose money.
As the pricing of health care becomes more and more centralized and standardized, there will be more examples where the prices are set too low and providers will walk away. Where lower cost providers can fill the void, that will happen. In some cases it will make little or no difference in terms of patient outcomes. Services of some sort will be rendered, likely of lower quality.
It is difficult to predict specific highly undesirable outcomes. Perhaps large segments of care will simply cease to be available and no one will notice. What is an almost certainty is there will some realms of care which will be tragically under-reimbursed, which will disappear, and have huge impact. The opportunities for this outcome are so great that it is a virtual certainty.
So what will Washington state do if the pharmacy which provides the lion's share of medication dispensing pulls the plug? At least they have some warning. How will other states respond when the the threat is a decentralized one and they wake up one day with no primary care doctors accepting new "insured" patients? Legislatively concocted rights to health care assume that there will always be sufficient resources that can be allocated to fulfill these moral obligations which have been converted to legal ones.
There are always legitimate needs and wants which go unfulfilled because scarcity is a fact of our world. Create punishing mandates to obligate people and businesses to provide services for payments less than the cost and it is the magic formula to make things even scarcer. Unless you can or want to hold a gun to their heads they will walk away. If Walgreens walks away, the state will likely save lots of money be stinting on services. At least everyone (or at least nearly everyone) will have insurance coverage.
Thursday, January 14, 2010
The Lord (Federal Government) Gave, and the Lord (Federal Government) Hath Taken Away
Harvard must be feeling like Job. Its endowment has taken a hit larger than the total actual endowments of of the the sum of all institutions not in the top 100. Now Harvard is the target of an IRS audit which is focused on some of the more profitable activities of this non-profit institution. See http://www.thecrimson.com/article/2010/1/13/harvard-irs-hmc-compensation/
I actually have a problem with this definition. What exactly is a non-profit? I looked to the source of all knowledge, Wikopedia to provide some insight.
Harvard has no stockholders, so what is the problem? The problem appears to be that the investment activities which Harvard leveraged into a tidy sum. Being shrewd about investment of endowment monies should be viewed as good stewardship of resources unless it actually crosses the line into something legally suspect.
However Harvard, like its other brother and sister institutions which have benefited from the tax status benefits conferred upon non-profits, long ago made a deal with the state. Now that non-profits such as Harvard look like fat cats by virtually any measure, it should come as no surprise that the cash hungry Feds see an opportunity to tap into a windfall. Large research institutions like Harvard have double exposure in that they receive substantial funds from the Federal government through grants and are exempt from taxes. Although I can only guess as to the exact amounts, add to this the cash flow into the health care businesses which comes from Medicare and Medicaid and I strongly suspect that the lion's share of money which is required to operate this institution comes either directly or indirectly from the Federal government.
This a cautionary tale. Build a business whose income stream is poorly diversified and it is an open invitation to be held hostage. The Harvard model is by no means unique. If the Feds find they can bully Harvard (and I think this is highly likely), it is going to send a chill throughout academia. What to do? What behavior do you need to change? Do you fire your investment advisors if your return is too good? Discard the charade of non-profit status and perhaps operate like the motion picture industry?
I actually have a problem with this definition. What exactly is a non-profit? I looked to the source of all knowledge, Wikopedia to provide some insight.
"A nonprofit organization (abbreviated NPO, also not-for-profit[1]) is an organization that does not distribute its surplus funds to owners or shareholders, but instead uses them to help pursue its goals.....A primary difference between a nonprofit and a for-profit corporation is that a nonprofit does not issue stock or pay dividends and may not enrich its directors. However, like for-profit corporations, nonprofits may still have employees and can compensate their directors within reasonable bounds."
Harvard has no stockholders, so what is the problem? The problem appears to be that the investment activities which Harvard leveraged into a tidy sum. Being shrewd about investment of endowment monies should be viewed as good stewardship of resources unless it actually crosses the line into something legally suspect.
However Harvard, like its other brother and sister institutions which have benefited from the tax status benefits conferred upon non-profits, long ago made a deal with the state. Now that non-profits such as Harvard look like fat cats by virtually any measure, it should come as no surprise that the cash hungry Feds see an opportunity to tap into a windfall. Large research institutions like Harvard have double exposure in that they receive substantial funds from the Federal government through grants and are exempt from taxes. Although I can only guess as to the exact amounts, add to this the cash flow into the health care businesses which comes from Medicare and Medicaid and I strongly suspect that the lion's share of money which is required to operate this institution comes either directly or indirectly from the Federal government.
This a cautionary tale. Build a business whose income stream is poorly diversified and it is an open invitation to be held hostage. The Harvard model is by no means unique. If the Feds find they can bully Harvard (and I think this is highly likely), it is going to send a chill throughout academia. What to do? What behavior do you need to change? Do you fire your investment advisors if your return is too good? Discard the charade of non-profit status and perhaps operate like the motion picture industry?
Monday, January 11, 2010
Triangulation may work for politics but not for love or health care
There is something fundamental about human interactions which is facilitated by the simplicity of just two parties. Let us look at love. There is no concept more complicated or unworkable as a love triangle. Granted there may be societies where polygamy rules, but I suspect this is because it is not about love. Throw love into the equation and a triangle becomes simply hopeless. Love involving two parties is complex. Love involving three parties becomes geometrically more complex and is essentially unworkable. People are almost always hurt.
In the beginning we had the physician and the patient, elegant in the simplicity of our relationship. Doctors, until recently could not do much and commanded modest sums for their services. Still we were attentive to our patients and we were respected by them in general. In the mid 20th century, the medical revolution took hold. We commanded even more respect from our patient although we were a less cheap date. To offset some costs we allowed a third party to enter into some of our transactions, the insurer. No big deal, our relationship with our patients was not affected substantially.
Roll forward to the new millennium. From it's modest roots, the relationship of doctors and patients is now thoroughly permeated with elements of the triangles; doctor, patient, insurer; doctor, patient healthcare system; doctor, insurer, healthcare system; patient, healthcare system, insurer; doctor, government, patient; insurer, healthcare system, government. Who loves whom? Who is beholden to whom? Whose money is it?
There is no question, love triangles can get very ugly. They involve control, money, love, respect, and autonomy. Triangles involving health care involve control, money, love, respect, autonomy and often health. We are fooling ourselves if we believe the long and clumsy arm of the state can domesticate these types of triangles. Reform as now offered serves us a more complex solution for a present system marked by unworkable complexity creating more vested parties and the replacement of love triangles with quadrangles, pentagons, and heptagons.
Yikes!
In the beginning we had the physician and the patient, elegant in the simplicity of our relationship. Doctors, until recently could not do much and commanded modest sums for their services. Still we were attentive to our patients and we were respected by them in general. In the mid 20th century, the medical revolution took hold. We commanded even more respect from our patient although we were a less cheap date. To offset some costs we allowed a third party to enter into some of our transactions, the insurer. No big deal, our relationship with our patients was not affected substantially.
Roll forward to the new millennium. From it's modest roots, the relationship of doctors and patients is now thoroughly permeated with elements of the triangles; doctor, patient, insurer; doctor, patient healthcare system; doctor, insurer, healthcare system; patient, healthcare system, insurer; doctor, government, patient; insurer, healthcare system, government. Who loves whom? Who is beholden to whom? Whose money is it?
There is no question, love triangles can get very ugly. They involve control, money, love, respect, and autonomy. Triangles involving health care involve control, money, love, respect, autonomy and often health. We are fooling ourselves if we believe the long and clumsy arm of the state can domesticate these types of triangles. Reform as now offered serves us a more complex solution for a present system marked by unworkable complexity creating more vested parties and the replacement of love triangles with quadrangles, pentagons, and heptagons.
Yikes!
Sunday, January 10, 2010
The Health Care Bubble
I read the book "Bailout Nation" by Barry Ritholtz. It is a very interesting history which takes a somewhat different perspective from the book "Demons of our own design" by Richard Bookstaber which focuses on the blindspots created by the Wall Street Quants whose models where believed to allow for investors to avoid risk. Ritzholtz both assigns blames to a host of parties and identifies an issue separate from the all of the exotic financial instruments which Bookstaber describes.
Beside having nothing but utter contempt for Allan Greenspan as Fed Chairman, Ritholtz takes aim on the problem with asset inflation which developed as a consequence of the ridiculous free money policy which marked Greenspan's tenure as Fed Chief. Cheap money drove home prices up and stimulated speculation on further asset growth. The underlying assets grew in value beyond the actual use value obtained.
The housing bubble has burst. It will not be re-inflating again anytime soon despite pumping huge amounts of capital into real estate. Buyers will not be so stupid to purchase these assets at inflated values. Even the government cannot possibly pump enough money into this segment of the economy and the foreign money that participated has moved elsewhere.
Where is the next bubble? Where have stupid subsidies and tax breaks been piled into a segment of the economy and driven prices upward to absurd and unsustainable levels? Where has investment been made based upon the assumption that despite large debt service the cash flows will be more than adequate to make the investments profitable? What business is both highly leveraged and heavily dependent upon a tax favored status of its business and incomes streams, which could be reversed by legislative fiat?
The answer seems obvious. It is the health care industry. Health care costs are increasing at more than twice the background level of inflation. Like the Federal Reserve, state and national governments are pumping increasingly larger sums of money into the health care economy. On top of this are the increasing sums from private insurers. Health care reform or no health care reform, this increasing cash infusion is coming to a stop. The results are predictable. We will see a deflation of the health care bubble. As the pressures to reign in costs become more pressing, the favored tax status of a variety of funds flows will be lost, thus shrinking cash infusions even more.
When this bubble bursts, the asset values which will be deflated will be both physical and human assets. Valuable technology will that which allows doctors and hospitals to get better outcomes for less. GE and Seimens will need to figure out how to make those scanners for less. As less money is pumped into health care, payment for professional services will be cut. Like the housing bubble, those who leveraged themselves to get in late will be hurt the worst. Medical students with hundred's of thousands of debt will discover they have made bad investments. Practices who leverage themselves to buy expensive equipment will find they cannot cover their debt service.
Who will be hurt? Perhaps a more important question is will patients be hurt? In the short term likely yes, some will. Physicians will need to change their expectations. I suspect that something different will arise from the ashes of the system which will be substantially disrupted. "Coverage" will mean something different. What actual care is delivered and by whom will likely bear scant semblance to what we have now. Hold on..it is going to be wild ride!
Beside having nothing but utter contempt for Allan Greenspan as Fed Chairman, Ritholtz takes aim on the problem with asset inflation which developed as a consequence of the ridiculous free money policy which marked Greenspan's tenure as Fed Chief. Cheap money drove home prices up and stimulated speculation on further asset growth. The underlying assets grew in value beyond the actual use value obtained.
The housing bubble has burst. It will not be re-inflating again anytime soon despite pumping huge amounts of capital into real estate. Buyers will not be so stupid to purchase these assets at inflated values. Even the government cannot possibly pump enough money into this segment of the economy and the foreign money that participated has moved elsewhere.
Where is the next bubble? Where have stupid subsidies and tax breaks been piled into a segment of the economy and driven prices upward to absurd and unsustainable levels? Where has investment been made based upon the assumption that despite large debt service the cash flows will be more than adequate to make the investments profitable? What business is both highly leveraged and heavily dependent upon a tax favored status of its business and incomes streams, which could be reversed by legislative fiat?
The answer seems obvious. It is the health care industry. Health care costs are increasing at more than twice the background level of inflation. Like the Federal Reserve, state and national governments are pumping increasingly larger sums of money into the health care economy. On top of this are the increasing sums from private insurers. Health care reform or no health care reform, this increasing cash infusion is coming to a stop. The results are predictable. We will see a deflation of the health care bubble. As the pressures to reign in costs become more pressing, the favored tax status of a variety of funds flows will be lost, thus shrinking cash infusions even more.
When this bubble bursts, the asset values which will be deflated will be both physical and human assets. Valuable technology will that which allows doctors and hospitals to get better outcomes for less. GE and Seimens will need to figure out how to make those scanners for less. As less money is pumped into health care, payment for professional services will be cut. Like the housing bubble, those who leveraged themselves to get in late will be hurt the worst. Medical students with hundred's of thousands of debt will discover they have made bad investments. Practices who leverage themselves to buy expensive equipment will find they cannot cover their debt service.
Who will be hurt? Perhaps a more important question is will patients be hurt? In the short term likely yes, some will. Physicians will need to change their expectations. I suspect that something different will arise from the ashes of the system which will be substantially disrupted. "Coverage" will mean something different. What actual care is delivered and by whom will likely bear scant semblance to what we have now. Hold on..it is going to be wild ride!
Wednesday, January 6, 2010
Caring vs. Doing
We are at a branch point for change in medicine. While the big lights are focused on the halls of Congress, I am not sure that is where the drivers of the big changes will be. The fundamental changes which is is evolving in medicine can be summarized by asking one question. What will be the primary mission of physicians vs. other health care workers? Will the primary mission of most physicians be to take care of patients or will their mission primarily be to do specific things to patients?
During my practice lifetime I have seen a dramatic movement toward the latter. In retrospect, this is not surprising since the payment system for physicians rewarded us for doing things to patients. Add to this the movement toward specialty medicine where we are increasingly rewarded for becoming more focused and less capable for the general caring role.
Nature abhors a vacuum and the vacuum relating to caring for patients are being filled by non-physicians. There may be some limited resistance from organized medicine but most of these caring activities represent lower margin business. I can't help but relate back to Clayton Christenen's observations that disruptive new entires generally move into lower margin activities and quickly end up displacing those who previously occupied such niches.
The future appears clear to me. In the not to distant future, physicians will relegate their roles as caring for patients. Assuming this happens, the question I raise how will this change how we educate physicians. For professionals increasingly deployed to do very specific and focused tasks, what is the utility of lengthy, expensive, and broad training which is promptly forgotten?
During my practice lifetime I have seen a dramatic movement toward the latter. In retrospect, this is not surprising since the payment system for physicians rewarded us for doing things to patients. Add to this the movement toward specialty medicine where we are increasingly rewarded for becoming more focused and less capable for the general caring role.
Nature abhors a vacuum and the vacuum relating to caring for patients are being filled by non-physicians. There may be some limited resistance from organized medicine but most of these caring activities represent lower margin business. I can't help but relate back to Clayton Christenen's observations that disruptive new entires generally move into lower margin activities and quickly end up displacing those who previously occupied such niches.
The future appears clear to me. In the not to distant future, physicians will relegate their roles as caring for patients. Assuming this happens, the question I raise how will this change how we educate physicians. For professionals increasingly deployed to do very specific and focused tasks, what is the utility of lengthy, expensive, and broad training which is promptly forgotten?
The waiting game
The frantic activities of the Congress before Christmas have given way to a peculiar calm. Things will get revved up again when the health care bills from the House and Senate get thrown in the great merging maw. The question is what will happen?
I now have a sense that it is nearly impossible for anything of substance to come as a product of a possible fusion of these bills. I also believed there was no way the House and Senate would be able to pass anything prior to the end of 2008 which should serve as a caution for anyone who thinks I can predict the future, particularly the political future.
Assuming I am wrong and that the miracle workers in the joint House and Senate committee pull off the merger through some sort of magical process, what is this going to look like and what type of shock waves will be unleashed? Depending on the constitutional issues which may come into play and how the legislation is crafted, the opportunities for legal challenges will be created. It suspect that there will be a series of immediate legal challenges which will placed. It will get very interesting and perhaps very ugly.
The constraints required for merging the bills creates few opportunities to make a workable and constitutional bill. Each constraint represents a hard stop, veto opportunity. Cost constraints are not compatible with broad state Medicaid subsidies. Focused state underwriting welcomes constitutional challenges. No state underwriting will lead to loss of state support for the entire process. Similar rock, paper,scissor scenarios may develop in handling regulatory measures focusing on insurance returns and abortion policies. Measures required to create political coalitions that are essential to create compromises needed to maintain coalitions create law which welcomes legal challenge.
We are also presented with surreal time lines. The bills need to be merged meaning sections need to be harmonized and differences adjudicated. How many people need to touch and review the sticking points? How long will it take to create some sort of close to a final draft which then needs to be reviewed by all of the House and Senate? How in the world will all this happen in a transparent fashion before the State of The Union Address. Again, I express more disbelief. Am I the realist or just a nay-sayer (or both).
In the end this may all be irrelevant in the long run. There will be marked changes in the health care environment, independent and any reform that occurs through federal legislation. I do not wish for change to stop. That would be crazy. Our present system rewards many of the wrong things, stimulates overconsumption of expensive services, and will bankrupt us. The worst case scenario would be for federal reform to act as a barrier to positive change while accelerating our move toward bankruptcy.
At this point it is just a waiting game.
I now have a sense that it is nearly impossible for anything of substance to come as a product of a possible fusion of these bills. I also believed there was no way the House and Senate would be able to pass anything prior to the end of 2008 which should serve as a caution for anyone who thinks I can predict the future, particularly the political future.
Assuming I am wrong and that the miracle workers in the joint House and Senate committee pull off the merger through some sort of magical process, what is this going to look like and what type of shock waves will be unleashed? Depending on the constitutional issues which may come into play and how the legislation is crafted, the opportunities for legal challenges will be created. It suspect that there will be a series of immediate legal challenges which will placed. It will get very interesting and perhaps very ugly.
The constraints required for merging the bills creates few opportunities to make a workable and constitutional bill. Each constraint represents a hard stop, veto opportunity. Cost constraints are not compatible with broad state Medicaid subsidies. Focused state underwriting welcomes constitutional challenges. No state underwriting will lead to loss of state support for the entire process. Similar rock, paper,scissor scenarios may develop in handling regulatory measures focusing on insurance returns and abortion policies. Measures required to create political coalitions that are essential to create compromises needed to maintain coalitions create law which welcomes legal challenge.
We are also presented with surreal time lines. The bills need to be merged meaning sections need to be harmonized and differences adjudicated. How many people need to touch and review the sticking points? How long will it take to create some sort of close to a final draft which then needs to be reviewed by all of the House and Senate? How in the world will all this happen in a transparent fashion before the State of The Union Address. Again, I express more disbelief. Am I the realist or just a nay-sayer (or both).
In the end this may all be irrelevant in the long run. There will be marked changes in the health care environment, independent and any reform that occurs through federal legislation. I do not wish for change to stop. That would be crazy. Our present system rewards many of the wrong things, stimulates overconsumption of expensive services, and will bankrupt us. The worst case scenario would be for federal reform to act as a barrier to positive change while accelerating our move toward bankruptcy.
At this point it is just a waiting game.
Subscribe to:
Comments (Atom)